YELP Holistic First Business Plan Defined Terms YELP Holistic First Business Plan SWOT Analysis Executive Summary Deliverables And Costs Snapshot Page To Benchmark Techniques Defined Terms for Five YELP Business Plans
Interim Discussion Paper means Australia: the healthiest country by 2020 - A discussion paper prepared by the National Preventive Health Taskforce.
Australia: the healthiest country by 2020
A discussion paper prepared by the National Preventive Health Taskforce
(c) Commonwealth of Australia 2008
This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any process without prior written permission from the Commonwealth. Requests and inquiries concerning reproduction and rights should be addressed to the Commonwealth Copyright Administration, Attorney-General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 or posted at http://www.ag.gov.au/cca Internet sites. This work is copyright. You may download, display, print and reproduce this material in unaltered form only (retaining this notice) for your personal, non-commercial use or use within your organisation. Apart from any use as permitted under the Copyright Act 1968, all other rights are reserved. Requests and inquiries concerning reproduction and rights should be addressed to Commonwealth Copyright Administration, Attorney-General’s Department, Robert Garran Offices, National Circuit, Barton ACT 2600 or posted at http://www.ag.gov.au/cca
Acknowledgements
The discussion paper was prepared on behalf of th e National Preventive Health Taskforce
Professor Rob Moodie, Chair
Professor Mike Daube, Deputy Chair
Ms Kate Carnell AO
Dr Christine Connors
Mr Shaun Larkin
Dr Lyn Roberts AM
Professor Leonie Segal
Dr Linda Selvey
Professor Paul Zimmet AO
Ms Meriel Schultz - writer
With advice from th e following experts
Alcohol Tobacco
Professor Rob Moodie (Chair) Professor Mike Daube (Chair)
Professor Steve Allsop Ms Viki Briggs
Ms Kate Carnell AO Professor Simon Chapman
Mr David Crosbie Dr Christine Connors
Professor Margaret Hamilton AO Mr Shaun Larkin
Mr Todd Harper Ms Kate Purcell
Mr Michael Livingston Dr Lyn Roberts AM
Professor Robin Room Ms Denise Sullivan
Professor Leonie Segal Professor Melanie Wakefield
Dr Linda Selvey
Professor Paul Zimmet AO Ms Michelle Scollo - writer
Mr Brian Vandenberg - writer
Obesity
Dr Lyn Roberts AM (Chair)
Professor Paul Zimmet AO (Deputy Chair)
Ms Ange Barry Dr Marj Moodie
Professor Wendy Brown Professor Kerin O’Dea AO
Professor David Crawford Mr Terry Slevin
Dr Sharon Friel Associate Professor Susan Thompson
Dr Tim Gill Associate Professor Melissa Wake
Ms Michele Herriot Dr Peter Williams
Ms Jane Martin
Ms Tessa Letcher - writer and all Taskforce members
Supported by th e Australian Government Department of Health an d Ageing
The contributions made by the Population Health Strategy Unit, Publications Unit and Communications Branch are gratefully acknowledged
Foreword
from the Minister for Health and Ageing
As a nation we must recognise that doing more to stay healthy and well will be key to coping with the human and financial costs of chronic and preventable illness. The Rudd Government was elected on a platform that recognised that things need to be done differently in health care in the future. Prevention of illness and chronic disease is central to a sustainable health system and a fuller life for all members of the Australian community. Too often in the past, individuals, communities and governments have focussed on the immediate issues of treating people after they become sick. Whilst this will always remain vital, and there is much to do in this area, we cannot afford to limit our focus to treatment and ignore prevention. I established the Preventive Health Taskforce in April and tasked it with developing a comprehensive and lasting Preventive Health Strategy by mid 2009. In the first instance the Taskforce was asked to focus on how to reduce harm flowing from obesity, tobacco and alcohol. In order to develop this discussion paper, the Taskforce has reviewed Australian and international research to come up with its preliminary views on what interventions could be available to prevent illnesses.
In this discussion paper the Taskforce identifies a wide range of options, some of them contentious, that it considers would have a positive impact in preventing illness. Importantly, the Taskforce has thrown down a challenge to the community to respond to its work – and provide input. With which findings and suggestions do you agree? Which do you disagree with and why? Do you have alternative or better ideas, and if so what are they? All parts of the community have a role to play, be they individuals and families, communities and industry, and of course federal, state and territory governments. No one sector alone can deal with the prevention agenda – we must act in concert and take responsibility for actions within each of our domains. So your views will be vital to the next stage of development of a truly national prevention strategy. I encourage you to provide input at this important time.
I thank all Taskforce members for their work, and particularly the Chair, Professor Rob Moodie, for their effort and foresight in preparing this discussion paper – Australia the Healthiest Nation by 2020. The ball is now in your court.
I encourage everyone to read the discussion paper and submit their views to the Taskforce to help develop an exciting and constructive new prevention agenda for the decades to come.
NICOLA ROXON, MP
Minister for Health and Ageing
Invitation from the Chair
The title of this discussion paper sets a great challenge for us. To achieve it we will have to make major reductions in the diseases caused by obesity, tobacco and alcohol.
We have to ensure that all Australians will benefit, particularly those with the poorest health – Indigenous Australians, those in rural and remote Australia and those with least education and income.
We base our recommendations on the best evidence we have to date. We invite you to respond. As a nation, as local communities, as corporations, and as families and individuals what major changes are we prepared to make to improve our health? What new resources and efforts are we prepared to invest? We need to know what you think.
We hope you will join the challenge to make Australia the healthiest nation by 2020.
Rob Moodie
Chair,
National Preventive Health Taskforce
Contents
Acknowledgements i
Foreword – from the Minister ii
Invitation from the Chair iii
Executive summary vii
1 Introduction 1
1
.1 Raising the bar for prevention 11.2 Setting targets for obesity, tobacco and alcohol 2
1.3 Understanding the challenges 3
1.4 About prevention 3
1.5 A framework for prevention 5
1.6 Principles for Preventive health 5
1.7 Working together 8
2 The case for prevention: overweight and obesity 9
2.1 The scale of the epidemic 9
2.2 High-risk groups 10
2.3 The need for urgent action 10
2.4 The costs of overweight and obesity 11
2.5 Challenges 12
2.6 Halting the epidemic 13
2.7 Priorities for action 14
3 The case for prevention: tobacco 19
3.1 The current situation 19
3.2 Historical trends in mortality 20
3.3 High-risk groups 21
3.4 Benefits from reducing smoking levels 21
3.5 Challenges 21
3.6 Future outlook 22
3.7 Priorities for action 23
4 The case for prevention: alcohol 29
4.1 The current situation 29
4.2 Patterns of drinking 30
4.3 High-risk groups 32
4.4 Benefits of reform 32
4.5 Challenges 33
4.6 Future outlook 36
4.7 Priorities for action 36
5 Supporting prevention 43
5.1 Common aspects across obesity, tobacco and alcohol 43
5.2 Support structures 44
5.3 Major policy imperatives to strengthen support systems 45
6 Measuring performance 47
6.1 Choosing performance indicators 47
6.2 Monitoring the indicators 50
6.3 Setting targets 50
6.4 Governance and performance monitoring 50
6.5 The monitoring system 51
7 Conclusion 53
7.1 Towards a National Preventive Health Strategy 53
References 55
Executive summary
Australia: the Healthiest Country by 2020 - A discussion paper by the National Preventive Health Taskforce
The purpose of the paper:
Australia is by international standards a very healthy country. But if we are to bequeath our children the legacy of the world’s healthiest country, major reductions in disease caused by overweight and obesity, tobacco smoking and harmful consumption of alcohol are needed.
Combining these threats with the increasing disparities in health between Indigenous and non-Indigenous Australians, between city dwellers and rural and remote Australians and between rich and poor Australians, means we have a real challenge on our hands if we aspire to being the healthiest nation by 2020.
The discussion paper outlines the case for reform in our approach to the prevention of illness and the promotion of health. Major changes in the way we behave as individuals, as families, as communities, as industries, as states and as a nation will be required.
The solutions are not only about individual choice and personal responsibility but also about the role of governments, business and industry, and non-government organisations.
The ideas proposed in this paper are for all Australians, not just governments.
The aim of this paper is to test our overall targets and the initial recommendations we have developed, in order to inform and provoke discussion and debate between Australians about how these targets can be achieved.
Targets for the healthiest country
The Taskforce is convinced that we can achieve the following targets by 2020:
-
Halt and reverse the rise in overweight and obesity
-
Reduce the prevalence of daily smoking to 9% or less
-
Reduce the prevalence of harmful drinking for all Australians by 30%
Contribute to the ‘Close the Gap’ target for Indigenous people, reducing the 17-year life expectancy gap between Indigenous and non-Indigenous people[1]
The Taskforce
The National Preventive Health Taskforce was created in April 2008 by the Nicola Roxon MP, the Minister for Health and Ageing.
Established initially for a three-year period, the Taskforce will produce the National Preventive Health Strategy in June 2009, focusing on the primary prevention of obesity, tobacco and harmful consumption of alcohol. Because of the need to prioritise these concerns, other important areas of Preventive health such as mental health, injury, immunisation, sexual and reproductive health, and illicit substance use will be considered in the next phase of the Taskforce’s work in 2009.
The Taskforce has based its recommendations on the best evidence to date. The evidence supporting the case for change and proposed actions is set out in the paper and in three comprehensive technical reports available online at www.Preventivehealth.org.au .
The call for urgent, comprehensive and sustained action
The answer does not lie in short-term projects. In order to reach the whole community, we need highly effective public education and the cooperation of mass media. We need every kindergarten, school and university, every workplace and business, and every community and neighbourhood in Australia involved and committed to improving and maintaining their health and productivity.
Chronic diseases not only result in death and disease, they are also a massive economic burden on the community and the health system. We can no longer afford to wait until we get sick. The answer lies in Preventive action.
Consumer demand needs to be redirected towards healthier choices. This can be achieved by industry producing, promoting and marketing much healthier products. We also need effective legislation and regulation, using pricing, taxation and subsidies as a means to encourage healthier choices. It could be suggested that the community is not yet ready for some of these ideas, but just think how unlikely it would have been 25 years ago to have introduced the approaches to tobacco control that are now commonplace.
In order to succeed, we need greatly enhanced monitoring, evaluation and research. Prevention programs need to reach the whole of the population and they must be given time to take effect. Changing the attitudes and behaviours of populations does not happen overnight.
Whose responsibility is Preventive health?
Our health is not only determined by our physical and psychological make-up and health behaviours, but also by our education, income and employment; our access to services; the place in which we live in and its culture; the advertising we are exposed to; and the laws and other regulations in place in our society.
Australia cannot become the world’s healthiest nation unless health becomes everyone’s business. Industry as supplier, marketer and employer; unions; the media as promoter; community and non-government organisations; philanthropists; academe – they all have influential roles to play. Similarly, all governments – local, state and federal across many sectors, led by the health sector – have distinct roles.
Prevention must become the business of state and federal Treasuries, and of leaders in the private sector.
We must be an inspiration to others: to early learning centres, schools and universities; urban planners; the sports and recreation industries; public transport and infrastructure; agriculture; police and emergency services; and to the hospitality and entertainment industries.
Where the market is failing, governments need to act to protect our health – particularly the health of children and adolescents.
Standards need to be established, regulations imposed where necessary and consumer education provided.
Governments, industry, advertising and the media need to work to reshape consumer demand in favour of healthy choices, and to make those choices available and accessible.
Healthier choices could include lower-alcohol beverages and lower-energy nutrient-rich foods and drinks.
Given the huge preventable losses of workplace productivity due to obesity, tobacco and alcohol, the private and public sectors have key roles as employers and in the promotion of much healthier workplaces. The experience of the new WorkHealth program in Victoria provides an immediate example from which we can all learn.
While Australia’s health care system plays a pivotal role in prevention, it requires better support and training in order to deal with these new challenges.
The National Health and Hospitals Reform Commission and the External Reference Group for the Primary Health Care Strategy are working on ways of ensuring that prevention is more effectively carried out across the health system as a whole, and in the primary health care system in particular. [Biographical information about members of the ERG]
Ultimately, it is communities, families and individuals who must change behaviours if we are to become a healthier nation.
Inequities in health
Major health inequities exist not only between Indigenous Australians and non-Indigenous Australians, but between rich and poor, and between rural and city dwellers. Even within a city such as Melbourne, life expectancy can vary by up to five years within a matter of kilometres.[2]
The World Health Organization’s Commission on the Social Determinants of Health makes three overarching recommendations to tackle the ‘corrosive effects of inequality of life chances’:
-
Improve daily living conditions, including the circumstances in which people are born, grow, live, work and age.
-
Tackle the inequitable distribution of power, money and resources – the structural drivers of those conditions – globally, nationally and locally.
-
Measure and understand the problem and assess the impact of action.[3]
With respect to obesity, tobacco and alcohol, Australian governments at all levels have a role in funding and supporting programs in communities, schools and workplaces. These investments have to take into account the ’inverse care law‘ – that those with more get more, and those with less get less – and reverse it so that underserved communities receive the support and resources they need.
The choices we have to make
We do have choices – we can do nothing new or do little – but this will mean a great deal of premature illness, suffering and death, all of which are preventable. As is already being seen, it will mean the overloading of hospitals, health and welfare services, a situation made more acute by the ageing of the Australian population. Similarly, it will mean rising costs within the health system and losses in workplace productivity.
We need urgent and sustained action. Australia’s record in prevention has been outstanding in many areas such as tobacco, road trauma, cardiovascular disease, skin cancer and immunisations. These Preventive actions have been crucial in increasing our life expectancy, but they have required substantial long-term funding.
The certainty of what needs to be done varies between the three immediate priorities: tobacco, alcohol and obesity. We know what we need to do to get our smoking rates down. Much is known about measures to reduce the harm caused by alcohol and overweight and obesity, but there is more to be learned. However, our need for knowledge should not stop action – we must act now on the basis of what we know, following the best practice and advice available, and learning by doing.
The necessary actions to reduce tobacco smoking are clear. They include making cigarettes more expensive, eliminating all forms of promotion and marketing, and revitalising public education campaigns.
Lessons from tobacco control are instructive, but approaches to obesity and alcohol will differ as governments, industry and communities work together to reshape consumer demand and support individuals in exercising healthy choices. The emphasis will be on reshaping attitudes and behaviours, rather than prohibiting them.
Why the focus on obesity, tobacco and alcohol?
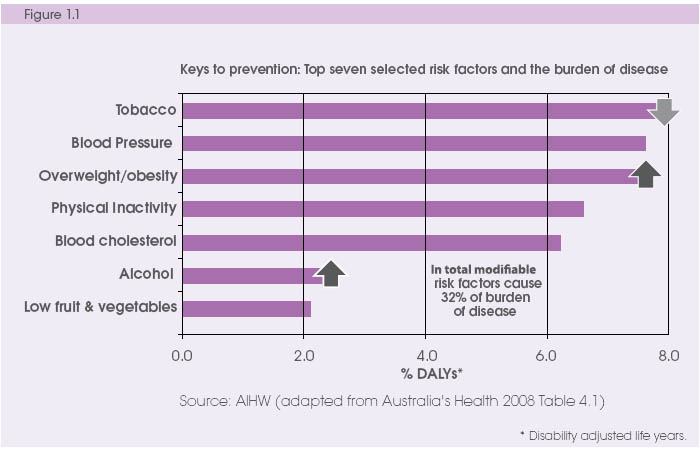
Put together, smoking, obesity, harmful use of alcohol, physical inactivity, poor diet and the associated risk factors of high blood pressure and high blood cholesterol cause approximately 32% of Australia’s illness.[4]
The World Health Organization estimates that, for many people, modifying these risk factors could help them gain an extra five years of healthy life.[5]
The prevalence of overweight and obesity in Australia has been steadily increasing over the past 30 years. In only 15 years, from 1990 to 2005, the number of overweight and obese Australian adults increased by a staggering 2.8 million. If the current trends continue unabated over the next 20 years, it is estimated that nearly three-quarters of the Australian population will be overweight or obese in 2025.
The National Children’s Nutrition and Physical Activity Survey 2007 indicates that almost a quarter of Australian children are overweight or obese, an increase from an estimated 5% in the 1960s. Nearly a third of children don’t meet the national physical activity guidelines. Only one-fifth of 4–8-year-olds and one-twentieth of 14–16-year-olds met the dietary guidelines for vegetable intake.
Recent trends in Australian children predict that their life expectancy will fall two years by the time they are 20 years old, setting them back to levels seen for males in 2001 and for females in 1997[6]. This is not a legacy we should be leaving our children.
As the following examples illustrate, if these health threats are left unchecked, our health systems will find it increasingly difficult to cope:
Type 2 diabetes is projected to become the leading cause of disease burden for males and the second leading cause for females by 2023, mainly due to the expected growth in the prevalence of obesity. If this occurs, annual health care costs will increase from $1.4 billion to $7 billion by 2032. [27]
Almost 2.9 million Australian adults smoke on a daily basis. Around half of these smokers who continue to smoke for a prolonged period will die early; half will die in middle age.[7] Smoking related illness costs up to $5.7 billion per year in lost productivity. [9]
The most recent national survey of drug use estimates that one in five Australians drink at a level that puts them at risk of short-term harm at least once a month. [64]
Almost three-quarters of Australians drink below levels for long-term risk of harm. However, among young adults aged 20–29 years, the prevalence of drinking at levels for long-term risk of harm is significantly higher (16%) than among other age groups.
The harmful consumption of alcohol not only causes problems for those who drink at risky levels but has repercussions across our society. Alcohol is involved in 62% of all police attendances, 73% of assaults, 77% of street offences, 40% of domestic violence incidents and 90% of late-night calls (10 pm to 2 am).[8]
The annual costs of harmful consumption of alcohol are huge. They consist of crime ($1.6 billion), health ($1.9 billion), productivity loss in the workplace ($3.5 billion), loss of productivity in the home ($1.5 billion) and road trauma ($2.2 billion).[9]
In total, the overall cost to the health care system associated with these three risk factors is in the order of almost $6 billion dollars per year, while lost productivity is estimated to be almost $13 billion.[9, 10]
Our focus on obesity, tobacco and alcohol is also due to two other important factors:
The burden of disease caused by obesity, tobacco and alcohol makes up a significant part of the 17-year difference in life expectancy between Indigenous and non-Indigenous Australians. Similarly, a large part of the differences in health status between rich and poor Australians and between city dwellers and rural and remote Australians can be attributed to obesity, tobacco and alcohol.
A relationship exists between growth and development during foetal and infant life and health in later years. Poor nutrition, cigarette smoking and alcohol use during pregnancy can result in long-term adverse health effects. Early life events play a powerful role in influencing later susceptibility to chronic conditions such as obesity, cardiovascular disease and type 2 diabetes.
What has prevention achieved?
In the 1950s three-quarters of Australian men smoked. Now less than one-fifth of men smoke. As a result, deaths in men from lung cancer and obstructive lung disease have plummeted from peak levels seen in the 1970s and 1980s. [4] Similarly, deaths from cardiovascular disease decreased dramatically from all-time highs in the late 1960s and early 1970s to today.
Road trauma deaths on Australian roads have dropped 80% since 1970, with death rates in 2005 being similar to those in the early 1920s. [4]
Australia’s commitment to improving immunisation levels has resulted in much higher immunisation coverage rates, eliminating measles and resulting in a decrease of nearly 90% in sero-group C meningococcal cases in only four years. These results have come about because of a 34-fold increase in funding over the last 15 years.
Deaths from Sudden Infant Death Syndrome (SIDS) have declined by almost three-quarters, dropping from an average of 195.6 per 100,000 live births from 1980 to 1990 to an average of 51.7 per 100,000 live births between 1997 and 2002.[11]
Prevention – a great investment
A study commissioned by the Department of Health and Ageing in 2003 showed quite spectacular long-term returns on investment and cost savings through the Preventive action of tobacco control programs, road safety programs and programs preventing cardiovascular diseases, measles and HIV/AIDS.[12]
For example this report estimated that the 30% decline of smoking between 1975 and 1995 had prevented over 400,000 premature deaths[13] and saved costs of over $8.4b, more than 50 times greater than the amount spent on anti-smoking campaigns over that period.
Prevention for a Healthier America shows that for every US$1 invested in proven community-based disease prevention programs (increasing physical activity, improving nutrition and reducing smoking levels), the return on investment over and above the cost of the program would be US$5.60 within five years.[14]What are some of the road blocks to progress?
There are a number of barriers to increasing the level of investment in effective prevention programs.
Despite the evidence, some influential people within the community still do not believe that prevention works, or that population-level behaviour change can occur.
Vested interests such as tobacco companies will do everything in their power to discredit or dilute prevention programs.
The effectiveness of Preventive methods has also been affected by variable popular demand. Results are not immediate, and it takes time before the benefits are seen by the community. The Taskforce sees prevention as an essential and complementary part of our national health system, and of our overall national infrastructure. It is now clear from the Australian 2020 Summit and the work of the National Health and Hospital Reform Commission that overall community support for Preventive approaches is increasing.
Prevention has sometimes been seen as ‘blaming the victim’, thus not endearing itself to the public.[15] It can also be seen as a means of controlling people’s behaviour if legislation or regulation are required, particularly where economic market forces fail. Unnecessary community antagonism to regulation can be successfully diminished over time, as has happened here and in many other countries with the introduction of legislation on tobacco advertising.
As noted earlier, our health behaviours are driven by a complex mix of social, economic and environmental forces – levels of income, education, employment, habits, customs, images and norms, advertising, prices of products, and so on. The Taskforce believes it is the role of governments to enable people to make the healthiest choices they can. However, those who believe that health behaviours result only from individual responsibility are much less inclined to see a role for regulation or effective, scaled-up public education.
Balanced, effective regulation and legislation, usually alongside effective and sustained public education, have been an essential element of most prevention programs to date.
Divided responsibilities can present real difficulties. For example, where the state and territory governments control liquor licensing and the Australian Government controls alcohol taxation, pricing and promotion. National leadership is needed, along with an increase in the capacity of monitoring, evaluation and research systems.
What do we need to do?
Obesity
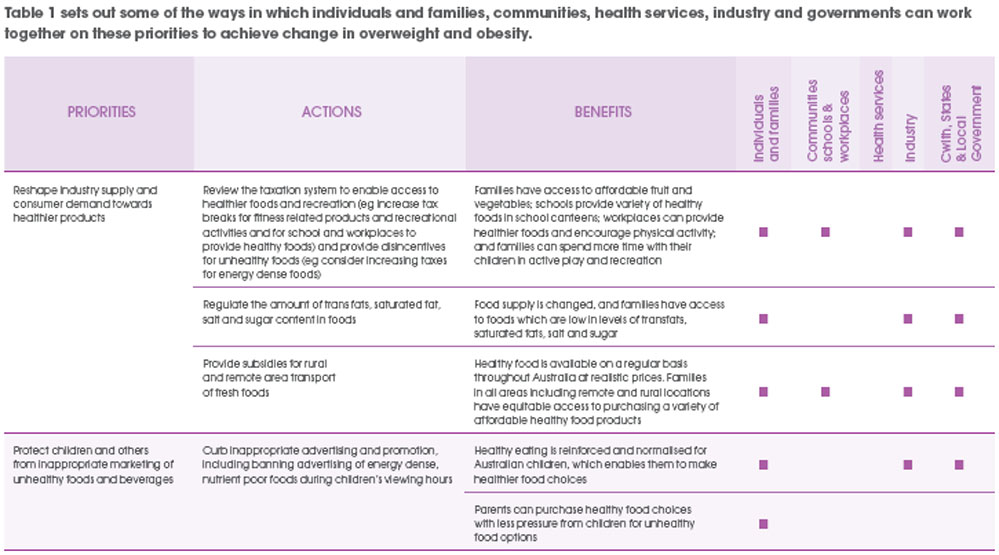
The Taskforce believes that in order to halt and reverse the rise in overweight and obesity the major actions are:
Food Matters).
Reshape industry supply and consumer demand towards healthier products by increasing availability and access to healthier food and activity choices and through the development of comprehensive national food policy (eg. modelled on the UK’s
Protect children and others from inappropriate marketing of unhealthy foods and beverages, and improve public education and information.
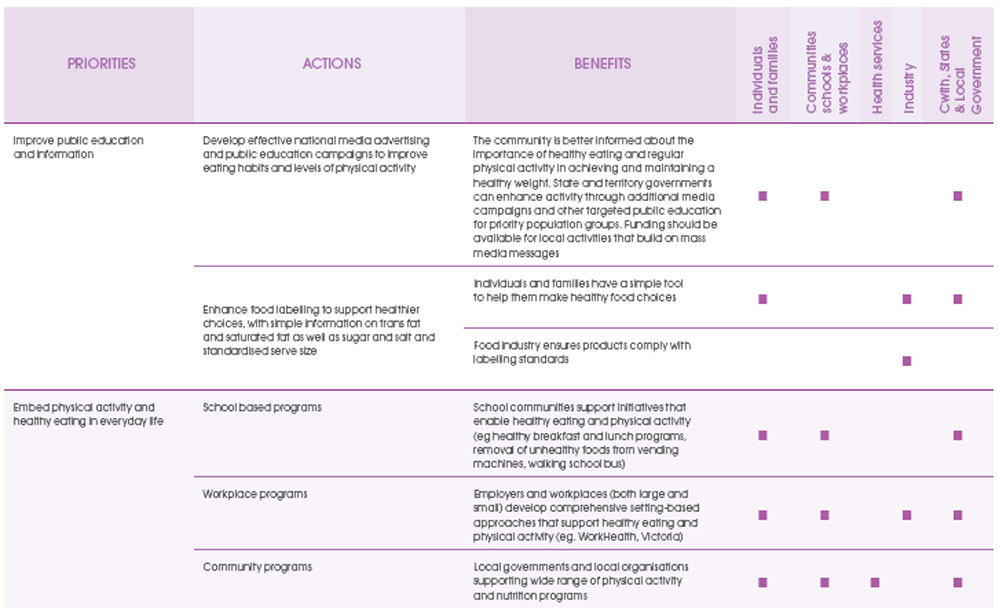
Embed physical activity and healthy eating in everyday life through school, community and workplace programs. At the same time these are reinforced by individuals and families choosing to become more active and to eat healthier foods.
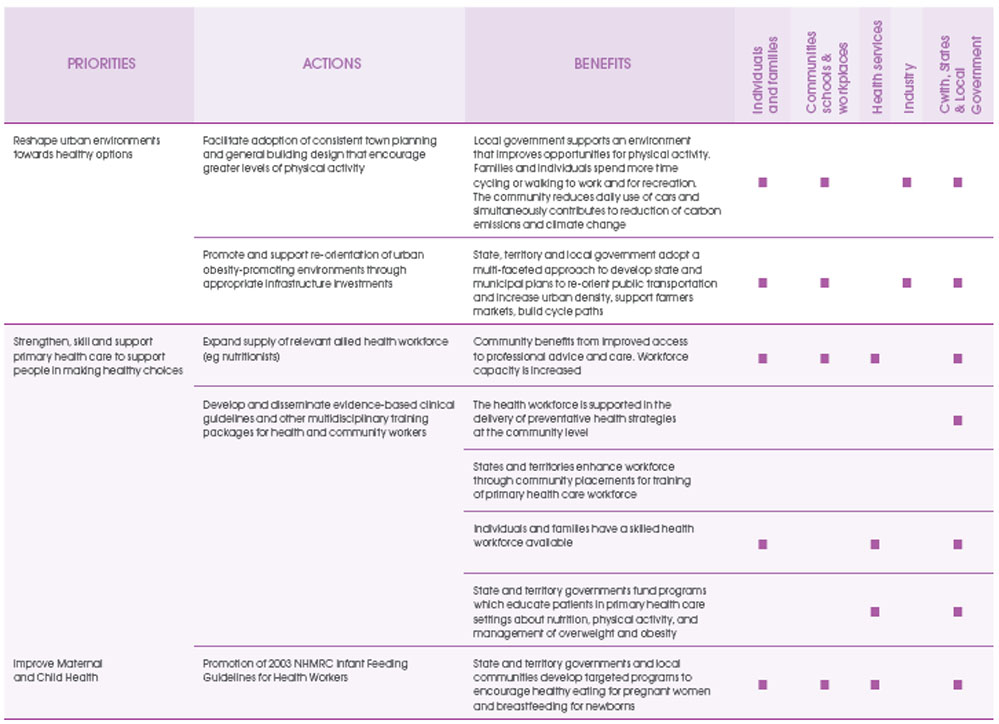
Reshape urban environments towards healthy options through consistent town planning and building design that encourage greater levels of physical activity and through appropriate infrastructure investments (for example, for walking, cycling, food supply, sport and recreation).
Strengthen, skill and support primary health care and the public health workforce to support people in making healthy choices, especially through the delivery of community education and advice about nutrition, physical activity and the management of overweight and obesity.
Close the gap for disadvantaged communities through the development of targeted approaches to overweight and obesity for disadvantaged groups, particularly Indigenous and low-income Australians, pregnant women and young children.
Build the evidence base, monitor and evaluate the effectiveness of actions.
Tobacco
The Taskforce believes that in order to reduce the prevalence of daily smoking to 9% or less, Australia needs to:
Ensure that cigarettes become significantly more expensive, and that efforts to achieve this through increases in excise and customs duty are not undermined by the increasing availability of products on which these duties have been evaded.
Further regulate the tobacco industry with measures such as ending all forms of promotion including point-of-sale displays and mandating plain packaging of tobacco products.
Increase the frequency, reach and intensity of education campaigns that personalise the health risks of tobacco and increase a sense of urgency about quitting among people in all social groups.
Ensure that all smokers in contact with any single part of the Australian health care system are identified and given the strongest and most effective encouragement and support to quit.
Ensure access to information, treatment and services for people in highly disadvantaged groups who suffer a disproportionate level of tobacco-related harm.
Increase understanding about how being a non-smoker and smoking cessation can become more ‘contagious’ – so that these processes can be accelerated among less well-educated groups and among disadvantaged communities.
Alcohol
The Taskforce believes that in order to reduce the prevalence of harmful drinking for all Australians by 30% the major actions are:
Reshape consumer demand towards safer drinking through:
Managing both physical availability (access) and economic availability (price). The high accessibility of alcohol – in terms of outlet opening hours, density of alcohol outlets and discounting of alcohol products – is an issue in many Australian communities. If managed well this leads to reduction in alcohol-related violence, injury, hospitalisation and death.
Addressing the cultural place of alcohol. Social marketing and public education are required, and will be more effective if the marketing of alcoholic beverages is restricted, including curbing advertising and sponsorship of cultural and sporting events.
Reshape supply towards lower-risk products through:
Changes to the current taxation regime that stimulate the production and consumption of low-alcohol products.
Improved enforcement of current legislative and regulatory measures (such as Responsible Serving of Alcohol or bans on serving intoxicated persons and minors, or continuing to lower blood alcohol content in drink-driving laws).
Removal of tax deductability for advertising and development of staged approach to restrict alcohol advertising.
Strengthen, skill and support primary health care to help people make healthy choices:
Support brief interventions as part of routine practice by health professionals and other health workers in primary health care settings to assist changes in drinking behaviour and attitudes to alcohol consumption.
Close the gap for disadvantaged communities:
There is a need for tailored approaches and services to reach Indigenous and other disadvantaged groups.
Improve the evaluation of interventions through:
Monitoring and evaluation of regulatory measures and other programs to underpin the further evolution of prevention strategies directed at inappropriate alcohol consumption.
Developing effective models of safer patterns of alcohol consumption in different communities trough changes to alcohol taxation arrangements, and an understanding of the impact of different types of alcohol outlets and their density on hospitalisation, violence and crime rates.
What action do we need for effective national prevention?
Inadequately funded or single, short-term and ad hoc projects and programs are unlikely to succeed. In fact, they may even be counter-productive, as they can give rise to an argument that ‘prevention doesn’t work’. Australia’s experience in immunisation, HIV/AIDS control and road trauma has demonstrated admirable returns on investment in Preventive action. The successful outcomes have eventuated, however, because of substantial and long-term funding, supporting well co-ordinated and well-directed national and state programs.
Separate infrastructure investments for efforts targeting each of the three risk factors will be costly. A robust ‘prevention support system’ is called for, including mechanisms for effective coordination across all strategies.
An essential component to enable effective action is to ensure leadership and coordination through the establishment of a National Prevention Agency.
At the national level, such an agency is needed to support the coordination of partnerships and interventions, ensure the relevance and quality of workforce training activities, effective social marketing and public education, and the monitoring and evaluation of interventions.
By bringing together expertise across the relevant areas, a national agency would provide leadership for the implementation of the National Preventive Health Strategy and build national prevention systems with strong capabilities.
Among its tasks, a national agency would:
Ensure the delivery of a minimum set of evidence-based, illness prevention/health promotion programs that are accessible to all Australians.
Engage key leaders and build new partnerships across federal, state and territory governments, national agencies, professional associations, local government, peak community groups, non government organisations, the private sector, the philanthropic sector and academia.
Commission and promote the uptake of new monitoring, evaluation and surveillance models for illness prevention.
Serve as an authoritative source of information on evidence, policy and practice.
Develop the evidence base on prevention through the design, implementation and evaluation of large-scale programs to improve the health and wellbeing of the population, or population sub-groups, by testing innovative strategies, programs and policies for illness prevention/health promotion.
Ensure the development of the necessary national workforce for illness prevention/health promotion, working with and through relevant national, state and local agencies to build capability in:
surveillance, prevention research, evaluation, economic impact research and modelling
social marketing and public education
legislation, regulation, economics and taxation
leadership and management.
Conclusion
We are constantly changing our behaviours. Just look at the changes in our nutrition, physical activity and smoking behaviours over the last 30 years. To be the healthiest country by 2020, and to have that good health shared by all Australians, will require substantial new shifts. There are no magic tablets in the laboratory.
It will require all of us as individuals and families to make healthier choices. It will also require industry, governments and community organisations to make healthier choices – whether it is the products they make and promote, or the policies, regulations and programs for which they are responsible.
Health is a fundamental human right. It is also, as the Prime Minister has pointed out, a major determinant of social inclusion, workforce participation, productivity growth and a potentially huge drain on the public and private purse. Get it right and literally everyone wins. Prevention is an essential element of getting it right.
Our invitation to you
This paper proposes a range of actions to improve our health in the three action areas of concern. The aim of the paper, and the ensuing consultation, is to seek community and stakeholder views on the framework and ideas we have developed. We invite you all – individuals, community groups, government and non government organisations and industry groups – to participate by making a submission on how we can make Australia the healthiest nation by 2020.
At the end of each chapter in the discussion paper, we propose a series of questions which will guide the Taskforce’s consultations and which we hope will be useful to guide your contributions. Please contribute to the Taskforce by using the form provided at the Taskforce website: www.Preventivehealth.org.au
Submissions will be accepted until 2 January 2009. The Taskforce will be holding meetings in each capital city and some major rural centres between October 2008 and February 2009. We hope you will join the challenge to make Australia the healthiest nation by 2020.
1. Introduction
In April 2008 the Minister for Health and Ageing, the Honourable Nicola Roxon MP, appointed a new National Preventive Health Taskforce to advise on the action needed in Preventive health for Australia, focusing on obesity, tobacco and alcohol as immediate priorities for action. The Taskforce, made up of health experts from around Australia, is to develop strategies to tackle health challenges caused by obesity, tobacco and alcohol and develop a National Preventive Health Strategy by June 2009 – the blueprint for Preventive health reform.
The strategy is to be directed at primary prevention, and will address all relevant arms of policy and all available points of leverage, in both the health and non-health sectors, in formulating its recommendations.
This discussion paper sets out the case for Preventive health reform and suggests a number of policy proposals, actions and support measures for obesity, tobacco and alcohol.
The paper raises some key questions that will form the basis of consultation, leading to the development of a National Preventive Health Strategy by June 2009.
1.1 Raising the bar for prevention
The challenge for Australia is to significantly ‘scale up’ prevention effort. This will start with three priority areas: reducing the growing epidemic of overweight and obese Australians, achieving a virtually smoke-free Australia, and combating the health and social harm resulting from risky drinking. Two specific factors have increased the momentum for a significant change in our approach to health: the national reform agenda of 2006 and the approach taken by the new government from late 2007.
Initiated by the Council of Australian Governments (COAG), the National Reform Agenda identified the crucial importance of better health to economic productivity and opened the way for a new whole-of government approach to health. COAG has established the Australian Better Health Initiative (ABHI), with the aim of refocusing the health system towards promoting good health and reducing the burden of chronic disease.
The Australian Government has decided to reorient Australia’s approach to the health system, with a much more vigorous strategy regarding prevention and greatly increased investment to prevent chronic disease. The Australian Government will:
‘treat Preventive health care as a first order economic challenge because failure to do so results in a long term negative impact on workforce participation, productivity growth and the impact on the overall health budget’.[16]
To achieve this end, the Taskforce is working closely with other groups involved in health reform. These include the National Health and Hospitals Reform Commission, whose priorities include looking at ways of ensuring a greater emphasis on prevention across the health system, and groups such as the National Primary Health Care Strategy, the Indigenous Health Equity Council and the National Advisory Council on Mental Health.
1.2 Setting targets for obesity, tobacco and alcohol
In the first instance, the Taskforce has been asked to provide advice in three specific areas: obesity, tobacco and alcohol. Each of these important public health risks is at a different point in its development. We know what works in tobacco control. We know much of what needs to be done to address alcohol problems, especially in terms of stemming intoxication and the social harms that result. The obesity epidemic is different. Australia is in the early stages of managing the rise in overweight and obesity prevalence – perhaps on a par with tobacco control 30 years ago.
Addressing these three very different areas and putting strong support systems in place will provide an important platform for future action in other areas such as mental health, injury, immunisation, sexual and reproductive health, and illicit substance use.
Measurable targets for 2020 for obesity, tobacco and alcohol:
By 2020 Australia can:
Halt and reverse the rise in overweight and obesity prevalence
Reduce the prevalence of daily smoking to 9% or less
Reduce the prevalence of harmful drinking for all Australians by 30%
Contribute to the ‘Close the Gap’ target for Indigenous people, reducing the 17-year life expectancy gap between Indigenous and non-Indigenous people[1]
Achieving these targets will require substantial community effort, leadership and new funding.
1.3 Understanding the challenges
Figure 1.1 (below left) shows how obesity, tobacco and alcohol (along with the related risks of physical inactivity, low-level consumption of fruit and vegetables, high blood pressure and high blood cholesterol) make up the top seven preventable risk factors that influence the burden of disease. The total of modifiable risk factors make up 32% of the burden of disease in Australia.[4]
The prevalence of smoking is declining too slowly; overweight and obesity and the harmful use of alcohol are escalating. The scale and pace of efforts in all these areas must be increased.
A number of other broad trends will have a continuing impact on the health and wellbeing of Australians and on our health system. These include:
The ageing of the population, which has important implications for health services usage and labour force participation.
1.4 About prevention
Well-planned prevention programs have made enormous contributions to improving the quality and duration of our lives. Prevention does work. We learned that from the great public health revolutions of the 19th century. While much remains to be done to prevent modern health problems, we have achieved major improvements through tobacco control, road trauma and drink driving, skin cancers, immunisation, Sudden Infant Death Syndrome (SIDS) and HIV/AIDS control.
In the 1950s three-quarters of Australian men smoked. Now less than one-fifth of men smoke. As a result, deaths in men from lung cancer and obstructive lung disease have plummeted from peak levels seen in the 1970s and 1980s. [4]
Similarly, deaths from cardiovascular disease have decreased dramatically from all-time highs in the late 1960s and early 1970s to today.
Road trauma deaths on Australian roads have dropped 80% since 1970, with death rates in 2005 being similar to those in the early 1920s. [4]
Australia’s commitment to improving immunisation levels has resulted in much higher immunisation coverage rates, eliminating measles and seeing a drop of nearly 90% in serogroup C meningococcal cases in only four years.
These have come about as a result of a 34-fold increase in funding over the last 15 years.
Deaths from Sudden Infant Death Syndrome (SIDS) have declined by almost three-quarters – dropping from an average of 195.6 per 100,000 live births from 1980 to 1990 to an average of 51.7 per 100,000 live births between 1997 and 2002.[4,11]
Prevention – a great investment
A study commissioned by the Department of Health and Ageing in 2003 showed quite spectacular, long-term returns on investment and cost savings from prevention – in tobacco control programs, road safety programs and programs preventing cardiovascular diseases, measles and HIV/AIDS.[12]
For example, this report estimated that the 30% decline in smoking between 1975 and 1995 had prevented over 400,000 premature deaths[13], and saved costs of over $8.4 billion, more than 50 times greater than the amount spent on anti-smoking campaigns over that period.[12, 13]
A recent US study
Prevention for a Healthier America: INVESTMENTS IN DISEASE PREVENTION YIELD SIGNIFICANT SAVINGS, STRONGER COMMUNITIES shows that for every US$1 invested in proven community-based disease prevention programs (increasing physical activity, improving nutrition and reducing smoking levels), the return on investment over and above the cost of the program would be US$5.60 within five years.[14] THIS USA REPORT SURPRISINGLY IGNORES THE COST SAVINGS FROM LIFESTYLE CHANGES WHICH REDUCE RECREATIONAL DRUG ABUSE, BECAUSE A Preventive HEALTH PROGRAMME WHICH INDUCES THE ABOVE IMPROVEMENTS WOULD ALSO REDUCE RECREATIONAL DRUG ABUSE WHICH WOULD ALMOST DOUBLE US$5.60 WITHIN 5 YEARS TO >US$11 FOR A US$1 OUTLAYThe World Health Organization (WHO) defines prevention as:
Approaches and activities aimed at reducing the likelihood that a disease or disorder will affect an individual, interrupting or slowing the progress of the disorder or reducing disability.
Primary prevention reduces the likelihood of the development of a disease or disorder.
Secondary prevention interrupts, prevents or minimises the progress of a disease or disorder at an early stage.
Tertiary prevention focuses on halting the progression of damage already done.
Effective prevention brings significant benefits to society as a whole, including improved economic performance and productivity.
Prevention has worked in Australia, from early public health legislation to more recent successes in areas such as road trauma, tobacco, HIV/AIDS, skin cancers, cardiovascular disease and childhood infectious diseases.
Prevention can:
Reduce the personal, family and community burden of disease, injury and disability
Allow better use of health system resources
Generate substantial economic benefits, which, although not immediate, are tangible and significant over time
Produce a healthier workforce, which in turn boosts economic performance and productivity (National Prevention Summit 2008)[17]
This includes a focus on health promotion, defined by WHO as
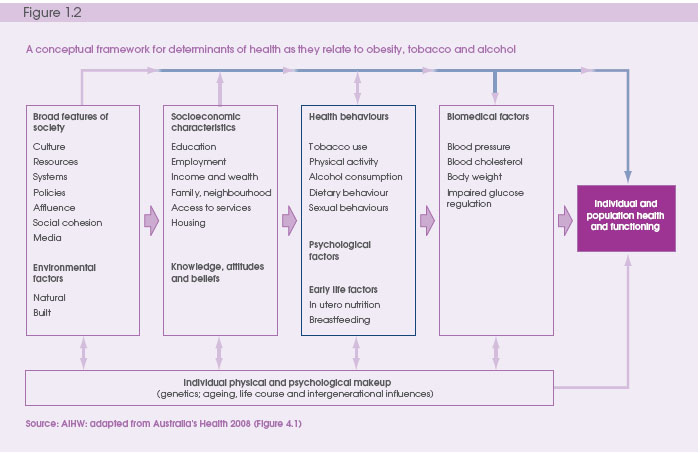
the process of enabling people to increase control over the determinants of health and thereby improve their health.[18]These determinants include the personal, social, economic and environmental factors (such as access to education, housing, employment, income) that influence the health status of individuals or populations (further described in
Figure 1.2 below).
1.5 A framework for prevention
A strong Preventive health strategy needs a framework that takes into account the key issues affecting Australians today, such as equity, health and the environment.
Figure 1.2 above is adapted from
Australia’s Health 2008[4] and shows the way in which the determinants of health relate to obesity, tobacco and alcohol, and to individual and population health and functioning.A recent report from the World Health Organization Commission on the Social Determinants of Health shows that health inequities (unfair, unjust and avoidable causes of ill health)
between countries also occur within countries. The report shows that, in general, the poor are worse off than those who are less deprived. The less deprived are in turn worse than those with average incomes, and so on.This slope linking income and health is the social gradient, and is seen everywhere – not just in developing countries – including the richest countries such as Australia.[19]
1.6 Principles for Preventive health
The following principles, based on those developed by the Health and Hospital Reform Commission, reflect what people in the community generally expect from an effective Preventive health system, and outline the principles that can guide effective action by governments.
The use of an agreed set of principles will help draw together the interests of different sectors in ensuring effective action and in developing an agreed National Preventive Health Strategy.
Community-driven principles
Strengthening prevention
People and family centred
Equity
Shared responsibility
Recognising broader environmental influences
Governance principles
Common frameworks
Comprehensive, staged approach taking
the long-term view
A mix of universal and targeted approaches
Combined approaches
Selected settings for action
A comprehensive support system
Community-driven principles
Strengthening prevention
Australia needs greater emphasis on helping people to stay healthy through a stronger investment in prevention, early detection and appropriate interventions to keep people in the best possible health.[20]
People and family centred
The direction of prevention should be shaped around the health needs of individuals, their families and communities. Responsiveness to individual differences, stage of life, cultural diversity and preferences through choice is important.[20]
Equity
Prevention activities should be accessible to all, based on health needs, not on an ability to pay.
Inequality arising from geographic location, socio-economic status, language, culture, Indigenous or ethnic status must be identified and addressed
.Shared responsibility
All Australians share responsibility for our health and the success of the health system.[20]
As individuals we each make choices about our lifestyle and behaviours; as a community we fund the health system; and as patients we make decisions about how we use the health system. The health system has an important role to play in helping people to become more self-reliant and better able to make the best choices to manage their own health needs.Business and industry both have important roles to play for obesity and alcohol, and governments have a responsibility to coordinate Preventive health reform, to deliver prevention programs and action, and to make sure adequate supports are put in place to enable individuals, families and communities and the health system to make useful contributions.
Recognise broader environmental influences
The environment plays an important role in our health and in helping to make sensible decisions about health. The environment is taken to include the global climate, the physical and built environment (for example, the workplace, air quality, planning decisions that affect our health), the socio-economic environment (including the working environment) and external influences, such as promotion of healthy or unhealthy behaviours.
Governance principles
Common frameworks
An international review of chronic disease prevention programs prepared for the Taskforce indicates that the use of a comprehensive framework is a common feature of prevention strategies. Important components of such a framework include:
a whole-of-society approach, including identification of high-risk population groups
a ‘life-course’ approach highlighting the needs of different groups as they move through different stages of their lives
a special focus on closing the health gap for disadvantaged groups
a concern for both individual and environmental risk factors and interventions
a commitment to improving the links between research, policy and practice
establishing a national coordinating body to set standards, drive and monitor Preventive health reform
diverse forms of partnerships to develop and implement innovative approaches
A comprehensive, staged approach taking the long-term view Prevention is most successful when comprehensive approaches are adopted, with multiple strategies. The priorities recommended in this discussion paper represent critical first steps in the roll-out of a comprehensive approach over time.
A mix of universal and targeted approaches Shifting population norms require small changes from everyone. Additional and different efforts are often required for disadvantaged populations, such as Indigenous Australians.
Addressing the health risks from obesity, tobacco and alcohol is one of the most important ways to close the health gap and improve the health of the wider community. In these, as in other areas, the targeting of health inequalities will require innovative and localised approaches within a broadly based universal prevention strategy.
Combined approaches
Multiple and long-term strategies are more effective than one-off programs. The mix of strategies needed will vary, depending on the area of focus. In particular, regulatory and educational approaches are often most effective when implemented together.
Selected settings for action
The settings within which people work, learn, live and play – schools, workplaces, neighbourhoods – provide valuable opportunities to promote health. Programs delivered in these settings should, where possible, adopt an integrated approach to risk factor reduction.
A strong support system
Prevention policies and programs require strong support systems and structures. These include linked components such as:
adequately funded and relevant research
comprehensive and relevant data collection systems
shared information across governments and other sectors
a strong surveillance system
a skilled and motivated workforce
effective national public education
locally identified mechanisms to establish and maintain partnerships and collaborations
1.7 Working together
Common approaches & collaboration
Effective prevention programs will depend on the participation of all Australian communities – in the cities, in the bush and in the remote areas of the country.
Australians as individuals will make prevention work. It is individuals who will take up regular physical exercise and make the right food choices for themselves and their families, who can voice a concern for public safety and an intolerance of drunken behaviour, and who can help make Australia a virtually smoke-free nation.
But individuals cannot achieve change on their own. They will need the support of employers and workplaces, unions, community leaders, industry, business and private sectors, the health services and all three levels of government.
Governments play a vital role in driving change and putting in place the support structures needed to achieve change. Genuine and sustained partnerships between the three levels of government are essential if Australia is to achieve the targets described in this paper.
In broad terms:
The Australian Government has responsibilities for policy and program coordination, across government policy, fiscal incentives and regulation, the development of a strong evidence base and practice guidelines, monitoring and surveillance systems and partnerships with national organisations, including employer and employee organisations and community agencies.
State and territory governments have responsibilities for legislation and regulation in their own sphere, coordination and programs throughout the community, across-government policy, partnerships with local governments and state-based non-government organisations, and monitoring and surveillance of the health of their population.
Local governments have responsibility for local planning and support structures. They play a vital part in engaging local communities, and in providing some of the services, amenities and programs that prevent illness and promote good health.
For the three tiers of government to work well together, excellent coordination of the respective roles and responsibilities will be required, along with clear accountability for all their activities and outcomes.
2020 target: halt and reverse the rise in overweight and obesity prevalence
2.1 The scale of the epidemic
One of the greatest public health challenges confronting Australia and many other industrialised countries is the obesity epidemic.
Australia is one of the most overweight developed nations, with overweight and obesity now affecting over 60% of Australian adults[21] and one in four children. The situation is worse for Aboriginal and Torres Strait Islander people, with nearly one in three Indigenous Australian adults obese.
The escalation of obesity prevalence is part of a worldwide trend linked to changing lifestyles, modernisation and technological change.
These changes affect the type and amount of energy-rich food we eat and our levels of daily physical activity. The increase in obesity over the past 20 years is a significant threat to Australia’s current levels of good health. It is already impacting on the healthcare system and threatens to reduce life expectancy for future generations. Tackling the obesity crisis and addressing diet, physical activity, maternal and child health and environmental factors must be a priority for prevention.
The major conditions for which obesity predicts higher mortality and/or morbidity include cardiovascular disease, type 2 diabetes, some cancers and, increasingly, osteoarthritis.
Obesity is also strongly associated with a wider range of conditions, including sleep apnoea and mental health, reproductive and back problems. Overweight and obese children and adolescents face some of the same health conditions as adults, and they may be particularly sensitive to the effects on self-esteem and peer-group relationships. For example, type 2 diabetes, previously rare in children and young adults, is now increasingly seen, particularly in the Indigenous community and in some newly migrating groups.
Diabetes prevalence is projected to increase two- to threefold over the next 25 years because of expected increases in the prevalence of obesity, along with demographic changes. Diabetes is also expected to cause the largest growth in disability in the elderly.
Current snapshot:
The prevalence of overweight and obesity in Australia has been steadily increasing over the last 30 years
The number of overweight and obese adults increased from 4.6 million in 1989–90 to 5.4 million in 1995, 6.6 million in 2001 and 7.4 million in 2004–05
Approximately 25% of children are overweight or obese, up from an estimated 5% in the 1960s
The mean body mass index (BMI) at which Australians enter adulthood has been gradually increasing over the last 20 years
The mean waist circumference increased between 2000 and 2005, and weight increase was most pronounced in young adults, particularly women[21]
2. The case for prevention: overweight and obesity
High body mass alone was responsible for 7.5% of the total burden of disease in 2003, including 20% of cardiovascular disease burden. High body mass and physical inactivity were responsible for 60% of the burden for type 2 diabetes)
Obesity is particularly prevalent among men and women in the most disadvantaged socio-economic groups, people without post-school qualifications, Indigenous Australians and among many people born overseas
The combined effect of the cluster of associated risk factors linked with obesity – poor diet, physical inactivity, high body mass and central (abdominal) obesity, high blood pressure and high cholesterol – is responsible for more than 50% of the total burden of cardiovascular disease
The total financial cost in Australia of obesity alone, not including overweight, was estimated at $8.3 billion in 2008 [10]
2.2 High-risk groups
Obesity is particularly prevalent among men and women in the most disadvantaged socio-economic groups, people without post school qualifications, Indigenous people and among many people born overseas.
While overweight and obesity are widely distributed among Australian adults and children, there are some significant variations in its distribution across the Australian population.
For Indigenous people, obesity is the second highest contributor to burden of disease after tobacco use.[22]
Adults born in Southern and Eastern Europe and those from the Oceania region are more likely to be overweight or obese (65% and 63% respectively).
Among school children, boys of middle Eastern and European background and boys and girls from Pacific Islander backgrounds are more likely to be obese.
People from certain ethnic backgrounds in Australia who are disproportionately more overweight or obese suffer higher rates of type 2 diabetes and cardiovascular disease.
2.3 The need for urgent action
Based on current trends there is an urgent and immediate need to address the growing prevalence of obesity and overweight in Australia.
Australia’s adult obesity rate is the fifth highest among OECD countries, behind the United States, Mexico, the United Kingdom and Greece.[23] While Australia’s mortality rates for coronary heart disease, stroke, lung cancer and transport accidents have improved significantly in terms of our ranking with other OECD member countries, this is not the case for our obesity ranking.
Assuming a constant increase in obesity prevalence over the next 20 years in line with current trends, the most recent projections are that there will be 6.9 million obese Australians by 2025.[10] Figures 2.1 and 2.2 below show this trend.
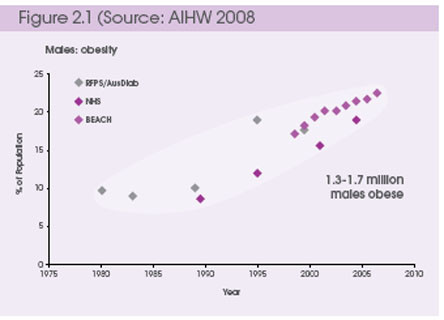 |
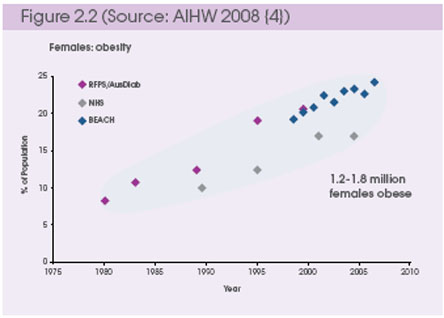 |
2.4 The costs of overweight and obesity
The total financial cost of obesity in Australia in 2008, not including overweight, is estimated at $8.3 billion. [10]
Reductions in the prevalence and incidence of overweight and obesity could realise savings not only to the health system but also to overall workplace productivity and a reduction in social costs. Of the total financial costs, the Australian Government bears over one-third (34% or $2.8 billion per annum) and state governments 5.1%.
This estimate includes productivity costs of $3.6 billion (44%), including short- and long-term employment impacts, as well as direct financial costs to the Australian health system of $2 billion (24%) and carer costs of $1.9 billion (23%).
Loss of ‘healthy life’ will be significant
Predictions of health loss (loss of healthy life) to the year 2023 indicate the largest projected increases will be for neurological disorders and diabetes, with a lesser increase for musculoskeletal disease. In comparison, rates of health loss are expected to decline for conditions such as heart disease, cancer, injuries and chronic respiratory conditions.[24]
The projected increase in rates of loss of healthy life associated with diabetes is due mainly to expected increases in body mass. Diabetes prevalence is projected to increase almost threefold over the next twenty years, and with higher rates of neurological conditions it is expected to cause the largest growth in disability in the elderly.[25]
Health expenditure will rise
A modelled case study prepared for the United Nations estimated that Australia’s total health expenditure will increase by 127% in the period 2002 to 2032, from $71 billion to $162 billion – an increase of $91 billion.[22] A study in the US found that if rising trends in obesity levels continue, as in Australia, disability rates will increase across all age groups, offsetting past reductions in disability – and that if this continued in the US, one-fifth of US healthcare expenditure would be needed for treating the consequences of obesity by 2020.[26]
Based on current trends:
Australians will continue to become more overweight and obese
There will be six million obese Australians by 2020 and 6.9 million by 2025[10]
The percentage of the Australian population who will be overweight or obese will have grown to a record 73% in 2025. This includes one-third of our children and three-quarters of our adult population[27]
Recent trends in Australian children predict that their life expectancy will fall two years by the time they are 20 years old, setting them back to levels seen for males in 2001 and for females in 1997[6]
A projected rise in the rates of type 2 diabetes, mainly due to expected growth in prevalence of obesity, will increase healthcare costs by $5.6 billion each year (from $1.4 to $7 billion) by 2032[27]
The burden of disease attributable to high body mass is likely to overtake tobacco as the leading preventable cause of burden as smoking rates decline[28]
2.5 Challenges
The challenges facing future prevention effort for overweight and obesity include:
Establishing effective leadership and coordination
The scale of the epidemic requires action to begin now. It is crucial that this involves all aspects of national, state and local governments, the non-government sector, industry, business, private interests and local communities, and across all levels of government and within and across sectors. Together, these key players must develop a staged approach that will sustain action in the long term, and will start by halting the current rise in the prevalence of obesity.
Shifting to a population-wide focus
If there is to be real change, Australia needs to avoid the natural tendency to focus only on individual and personal responsibility and ensure that policy directions to tackle overweight and obesity as a major public health issue have a population-wide focus.
A wide range of forces, some outside the control of individuals and families, interact to shape patterns of overweight and obesity. The magnitude of this problem warrants a stronger population-level response.
Equity
Targeted approaches are needed for groups with disproportionately high rates of overweight and obesity, including Indigenous people, people of different cultural backgrounds (particularly from Pacific Islands and the Middle East), people of lower socio-economic status, children and young or pregnant women.
Interventions aimed at children and pregnant women may have a significantly higher impact.
Working with industry
The contribution of Australian industry is crucial in tackling the obesity problem. Industry sectors have already demonstrated their willingness and ability to work in partnership with others to develop strategies and products to enhance the health of Australians. Industry (especially the food and beverage industry and restaurant and catering industries) can make an important contribution by providing information (for example, product and menu labelling and responsible marketing); placing healthy products in more prominent positions in supermarkets; improving the food supply (for example, making healthier and affordable food products available); and developing a more environmentally sustainable food chain.
Building the evidence base
It will be important to continue developing the evidence base for action on overweight and obesity, but this should not be a cause for delayed action. Australia can build a strong evidence base through research, evaluation, monitoring and surveillance. This should include a much higher investment in research and evaluation of interventions, as well as improving our understanding of the causes of obesity. A specific research agenda should be developed with appropriate levels of funding – public and private. This will need to be supported by the improved monitoring and harmonisation of surveillance systems across Australia.
Ensuring public safety
The weight loss industry in Australia is worth millions each year (for example, it is estimated that young women aged 18–32 years spent almost $414 million on managing their weight in 2002). There are a wide range of weight loss programs available, including commercial weight loss programs (such as pharmacy-based programs), internet-based programs, weight loss products (such as meal replacements) and community-based weight management or exercise groups. These programs are popular – but there is limited data on their effectiveness. To ensure that practices are safe and effective, programs need to be reviewed and a common code of practice for the industry needs to be developed.
2.6 Halting the epidemic
Reductions in the prevalence and incidence of overweight and obesity would lead to significant social and economic benefits for all Australians, including significant improvements in the health and wellbeing of individuals and families, substantial savings to the healthcare system and improvements in workplace productivity.
In addition to improvements in weight management and the prevention of weight gain in those already overweight or obese, the prevention of overweight and obesity provides an outstanding opportunity to realise a wide range of benefits. By encouraging healthy eating and a more physically active lifestyle across all age groups in the population, we can improve the health and wellbeing of individuals, reduce costs to society, maintain and improve the high levels of life expectancy Australians currently enjoy, and help to narrow gaps in life expectancy.
Investment in prevention not only benefits those who are already overweight or obese, but those who are currently at a healthy weight. Weight loss in people who are overweight and obese improves physical, metabolic, endocrine and psychological complications. Obesity-related mortality can be reduced through weight loss: even a modest loss of 5–10% of body weight can lead to significant health benefits.[29]
The benefit of acting now
The Australian healthcare system could save $1.5 billion annually if more people were physically active for 30 minutes a day (based on the gross cost of the prevention, diagnosis and treatment of medical conditions attributable to physical inactivity related to direct public and private health expenditure][30]
Weight loss in people who are overweight and obese improves physical, metabolic, endocrine and psychological complications. Obesity-related deaths can be reduced through weight loss – even a modest loss of 5–10% of body weight can lead to significant health benefits(24)
As well as helping in weight loss and the prevention of weight gain, being physically active can also help prevent type 2 diabetes, lower blood pressure, reduce the risk of some cancers and contribute to mental health wellbeing[28]
A healthier diet can help in the reduction of high blood fat (for example, cholesterol levels), one of the conditions placing significant pressure on the Pharmaceutical Benefits Scheme, as well as providing many other health benefits[28]
As BMI increases, so do length of hospital stay, medical consultations and use of medication.[31] Halting current increases in BMI will therefore assist in preventing associated cost rises
Strategies that are effective in halting and/or reducing the rise in population BMI will benefit national productivity. Obesity was associated with over four million days lost from Australian workplaces in 2001. Obese employees tend to be absent from work due to illness significantly more often than obese workers, and for a longer period of time, and they are less likely to be in the labour force[32]
For newly emerging areas of health risk – such as obesity – there are benefits from adopting a ‘learning by doing
’ approach.Obesity is a relatively new area for prevention globally. Australia is one of an early group of countries committed to making a concerted effort. We are at the beginning of a long journey to reverse the current situation, and 2020 will deliver only on the first steps in that journey.
Already, there is evidence about the interventions that are necessary to improve nutrition and physical activity. Lessons from other areas of successful action, such as tobacco control, HIV/AIDS and road trauma, are transferable to obesity.
While many pieces of this jigsaw are known, community readiness for a set of hard-hitting, multifaceted interventions on obesity may at this stage be similar to that in the early days of tobacco control.
There is also much evidence about the effectiveness of interventions that is yet to be captured. These factors speak to a ‘
learning by doing’ approach – that is, the staged trialling of a package of interventions accompanied by an appropriate allocation of resources as well as comprehensive monitoring and evaluation.The World Health Organization recommends the following actions:
legislate to support the healthier composition of food products
limit the marketing of food and beverages to children
enact fiscal policies to encourage the consumption of healthier food products
promote access to recreational physical activity
change physical environments to support active commuting and create space for recreational activity
create healthy school and workplace environments
undertake mass media, education and information campaigns to promote healthy diets and physical activity
offer health advice and Preventive services in primary healthcare settings[5]
2.7 Priorities for action
In the first instance, policy reforms should aim to halt and reverse the rise in the prevalence of overweight and obesity.
Major imperatives are to :
Reshape industry supply and consumer demand towards healthier products by increasing availability and access to healthier food and activity choices
Protect children and others from inappropriate marketing of unhealthy foods and beverages, and improve public education and information
Embed physical activity and healthy eating in everyday life through school, community and workplace programs
Reshape urban environments towards healthy options through consistent town planning and building design that encourage greater levels of physical activity and through appropriate infrastructure investments (for example, for walking, cycling, food supply and recreation)
Strengthen, skill and support primary health care to support people in making healthy choices, especially through the delivery of community education and advice about nutrition, physical activity and the management of overweight and obesity
Close the gap for disadvantaged communities through the development of targeted approaches to overweight and obesity for disadvantaged groups, particularly Indigenous and low-income Australians, pregnant women and young children
Build the evidence base, monitor and evaluate the effectiveness of actions taken
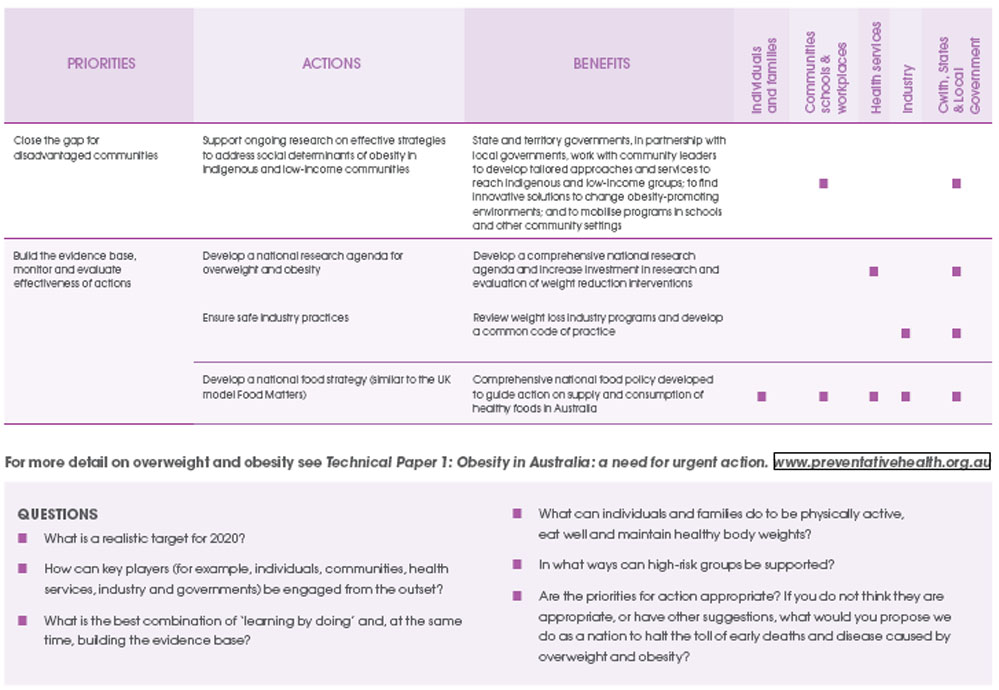
QUESTIONS
What is a realistic target for 2020?
How can key players (for example, individuals, communities, health services, industry and governments) be engaged from the outset?
What is the best combination of ‘learning by doing’ and, at the same time, building the evidence base?
What can individuals and families do to be physically active, eat well and maintain healthy body weights?
In what ways can high-risk groups be supported?
Are the priorities for action appropriate? If you do not think they are appropriate, or have other suggestions, what would you propose we do as a nation to halt the toll of early deaths and disease caused by overweight and obesity?
3. The case for prevention: tobacco
2020 target: reduce the prevalence of daily smoking to below 9%
Between 1950 – when clear evidence on the dangers of smoking became available[33, 34] – and 2008, more than 900,000 Australians died because they smoked.[35] This toll will exceed the million mark within a few years.
With a huge body of evidence now providing clear guidance on the most effective means of reducing smoking, both at the population level and in clinical settings, there is no reason to allow the smoking epidemic to continue for another 60 years.
If the prevalence of daily smoking is reduced to 9% or less by 2020, experts believe that smoking will continue to decline quite rapidly until it is no longer one of Australia’s major public health problems. This target is feasible, but achieving it will require a dramatic reduction in the number of children taking up smoking and a doubling of the percentage of smokers trying to quit.
Tobacco use is currently the single-biggest preventable cause of death and disease in Australia.[25, 36]
Smoking resulted in an estimated 15,511 deaths in 2003 and cost the Australian community around $12 billion in tangible net costs in 2004–05.[9] Tobacco use is responsible for 12% of the total burden of disease and 20% of deaths in Indigenous Australians.[22]
A report to the Department of Health and Ageing assessing the returns on investment in public health in Australia estimated that the 30% decline of smoking between 1975 and 1995 had already prevented over 400,000 premature deaths[13], and saved costs of over $8.4 billion.[12]
Modelling of the impact of reductions in smoking on healthcare expenditure indicates the potential for substantial further savings.
3.1 The current situation
Twenty-five years after the introduction of the first series of policies to discourage smoking, the use of tobacco products in Australia is at an historic low.
Figure 3.1 shows that the proportion of adult Australians who describe themselves as current smokers fell significantly between 1980 and 2007.[37]
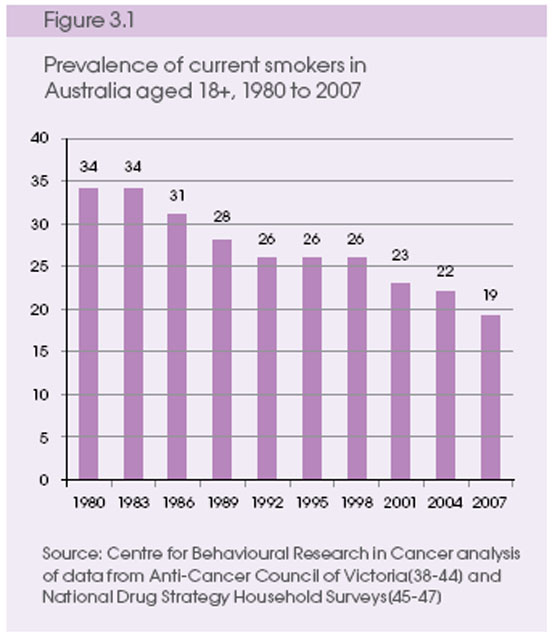
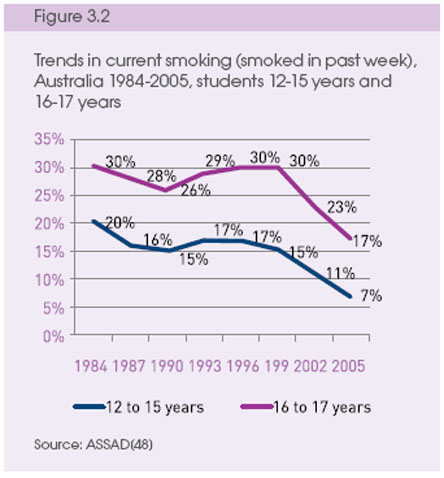
Figure 3.2 shows that the proportion of teenagers who smoke has fallen sharply since 1999.
3.2 Historical trends in mortality
Figures 3.3 and 3.4 show the downward trends of death from two tobacco-related diseases (lung cancer and chronic obstructive pulmonary disease) since comprehensive tobacco control policies were put in place in Australia, showing their success and the importance of maintaining strong tobacco control into the future. The landmark reports of the Royal College of Physicians of London and the US Surgeon General were released in 1962 and 1964. These are dramatic illustrations of the impact of Preventive programs, albeit over a much longer period than should have been the case.
The weight of tobacco levied for excise and customs duty has fallen steadily since 1975 and is currently lower than it has been at any time since records were first collected shortly after Federation.[49]
While Australia should be proud of its record, there is no cause for complacency.
Over three million people (around 18% of Australians aged 14 years and over) still smoke, with almost 2.9 million smoking on a daily basis.
About half of these smokers who continue to smoke for prolonged periods will die early, half of them in middle age when children and grandchildren depend on them and while they are in the most productive years of their working lives.[50]
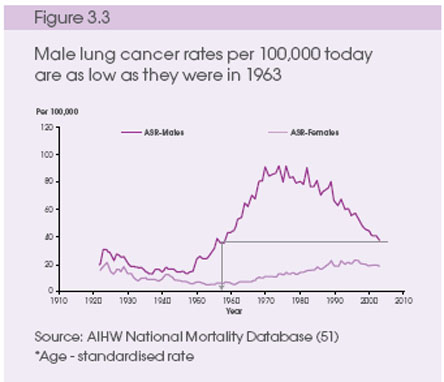 |
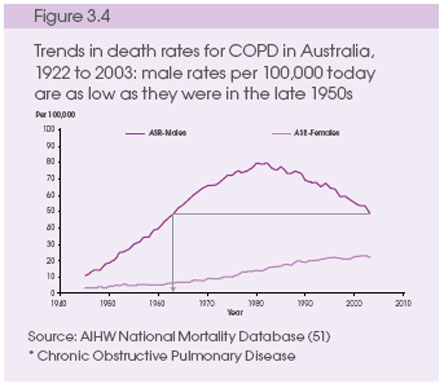 |
3.3 High-risk groups
Rates of smoking in high-risk groups differ from the general population.
Smoking rates are rapidly declining among the affluent, but continue to be substantially higher among those with lower levels of education and those living in more disadvantaged areas.
The decline in smoking rates among adults living in the most disadvantaged areas appears to have levelled off.[52]
Smoking rates among Indigenous Australians are more than double those in the rest of the community.[53]
Among children living in households where at least one person smokes, those who live in disadvantaged areas are almost four times more likely to be exposed to second-hand tobacco smoke indoors than children living in more affluent areas of Australia.[54]
Almost one in five pregnant women report smoking during pregnancy,[55] including 42% of teenagers and 52% of Indigenous women,[56] posing serious risks to the mothers, and long-lasting and far-reaching effects on their offspring.[57]
3.4 Benefits from reducing smoking levels
For every 1000 smokers who quit, at least 40 will be spared a diagnosis of chronic illness.
Most of the benefits from reducing the prevalence of smoking over the next decade will be realised in the 2030s and 2040s. However, even by 2020 we can expect to see savings in excess of our investments at both national and state levels. Modelling the impact on deaths and costs over just the next 10 years predicts that for every 1000 smokers who quit, at least 40 will be spared a diagnosis of chronic lung disease, lung cancer, heart attack or stroke, with significant healthcare savings.[58]
Benefits from reduced tobacco use go well beyond savings to the healthcare system.
Work for the Victorian Treasury indicates that if impacts on costs currently borne by the business sector were taken into account, the returns on investment in tobacco control would be even higher than current estimates. Accelerating the decline of smoking would bring benefits not only in public health but also in keeping people in the workforce longer, reducing absenteeism and
Increasing Productivity.Quitting smoking provides other benefits Quitting smoking provides extra funds in individual and family budgets that could be directed towards other household expenditure.
The levels of improved fitness that results from giving up smoking can help people to make other lifestyle changes.
Given that spending on tobacco products can increase financial stress, prevent the accumulation of wealth and contribute to the perpetuation of intergenerational poverty, tobacco control should be regarded not just as a health policy but also as a key strategy for the prevention of social disadvantage.
3.5 Challenges
A number of challenges still remain for tobacco control.
Loss of momentum in national and state efforts.
Despite progress in tobacco control over the past 30 years, there is no guarantee that the decline will continue. Prominent public education campaigns in some of the larger states have helped to drive a reduction of around 30% in total prevalence of smoking in Australia over the last 12 years.
However, there has been a ‘flattening out’ in the reduction in the prevalence of smoking rates in Australia, as the latest results of the National Drug Strategy Household Survey indicate.
Between 2004 and 2007 prevalence of weekly rates fell by only 1.1 percentage points (6%), compared to a drop of 2.1 percentage points (9%) over the previous three years.
Evidence from Australia and overseas shows that when tobacco control efforts stall, so does the decline in smoking. There is a danger of complacency, which we can ill afford in facing up to our largest preventable cause of death and disease.
Further reduction in smoking prevalence
Reducing smoking further requires a dramatic reduction in both the number of children taking up smoking and an increase in the number of people trying to quit. In Australia, the challenge is to halve the rate of smoking uptake and double the percentage of adult smokers who quit each year. If this could be achieved, smoking prevalence would reduce to 9% by 2020 and then continue to decline quite rapidly.
Clarifying roles of Commonwealth and state governments
In the early years, tobacco control in Australia was largely seen as the responsibility of state and territory governments. Differences in legislation and programs have resulted in children and adults in some jurisdictions being exposed to forms of tobacco marketing to which they are not exposed in others. In addition, smokers in some jurisdictions do not have access to services that are free in others.
The Australian Government has been more directly involved in some policy initiatives and, briefly, the National Tobacco Campaign, as well as ratifying the International Framework Convention on Tobacco Control in December 2003. It will be important that all jurisdictions recognise their responsibility and respond effectively.
Socio -economic disparities in tobacco use Complex, interacting factors drive disparities in the uptake and continuation of smoking, with people in highly disadvantaged groups suffering a disproportionate level of tobacco-related harm. We need to better understand the combination of reinforcing factors that perpetuate high smoking rates in disadvantaged groups and respond with suitable interventions based on appropriate consultation.
3.6 Future outlook
Australia has the capacity to:
Substantially reduce the affordability of tobacco products
Eliminate all remaining forms of promotion of tobacco, including marketing at the retail level
Establish a mechanism for the regulation of tobacco products
Licence all retailers and limit the number and type of retail outlets
Ensure no tobacco products are sold to children
Improve consumer information
Revitalise the National Tobacco Campaign
Protect the public (especially children) from exposure to second-hand tobacco smoke
Ensure appropriate programs and services for disadvantaged groups
Improve supports to quit smoking
These actions would halve the rate of smoking uptake, double the percentage of adult smokers who quit each year, and reduce the prevalence of daily smoking to 9% or less by 2020.
3.7 Priorities for action
If the prevalence of daily smoking is reduced to 9% or less by 2020, there are good grounds to believe that smoking will continue to decline quite rapidly until it is no longer one of Australia’s leading public health problems.
Achieving the 2020 target will require a dramatic reduction in the number of children taking up smoking and a doubling of the percentage of smokers trying to quit. To reach the target, it is vital to establish and maintain systems with enough capacity to sustain our good record in the reduction of smoking and exposure to second-hand smoke.
Extensive evidence internationally shows that the following five measures significantly reduce smoking:
raising tobacco taxes and prices
enforcing bans on tobacco advertising, promotions and sponsorship
warning people about the dangers of tobacco n protecting people from tobacco smoke
helping people to quit[5]
To achieve the 9% target, Australia Needs to address the following imperatives:
Ensure that cigarettes become significantly more expensive, and that efforts to achieve this through increases in excise and customs duty are not undermined by the increasing availability of products on which these duties have been evaded
Further regulate the tobacco industry with measures such as ending all forms of promotion including point-of-sale displays and mandating plain packaging of tobacco products
Increase the frequency, reach and intensity of education campaigns that personalise the health risks of tobacco and increase a sense of urgency about quitting among people in all social groups
Ensure that all smokers in contact with the Australian healthcare system are identified and given the strongest and most effective available encouragement and support to quit
Ensure access to information, treatment and services for people in highly disadvantaged groups who suffer a disproportionate level of tobacco-related harm
Increase the understanding about processes of social diffusion against smoking – how being a non-smoker and smoking cessation become more ‘contagious’ – so that these processes can be accelerated among less well-educated groups and disadvantaged communities
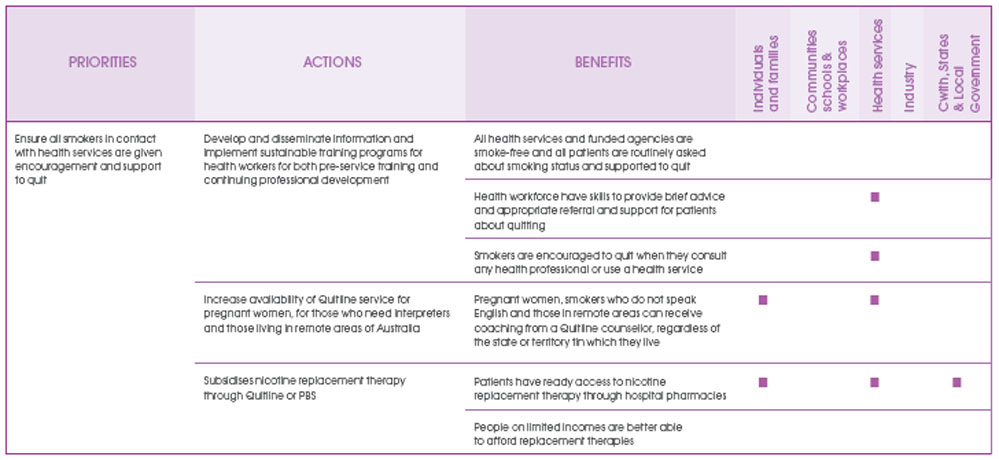
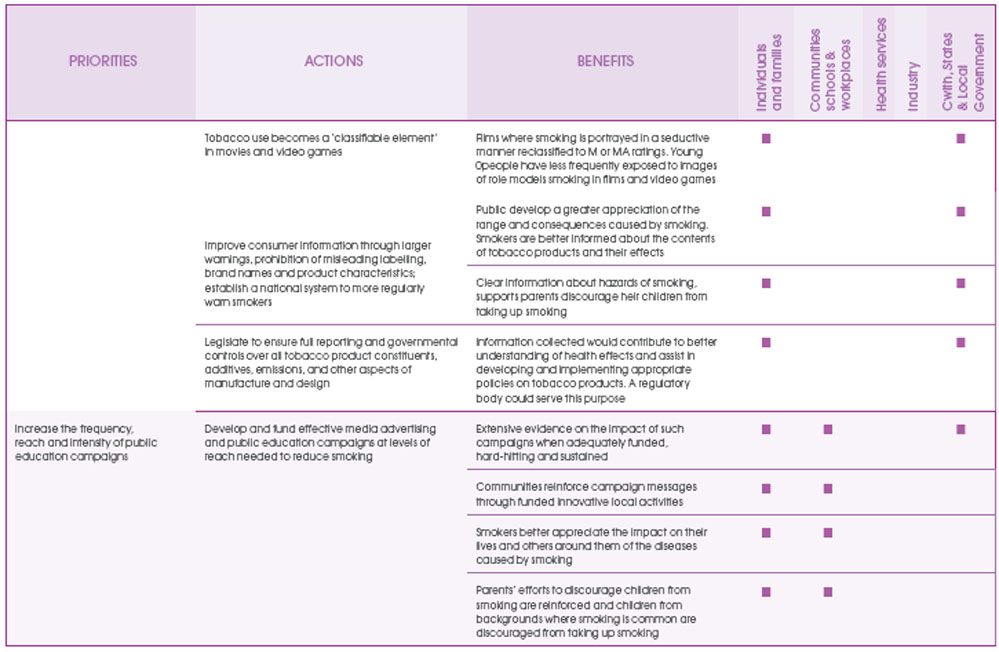
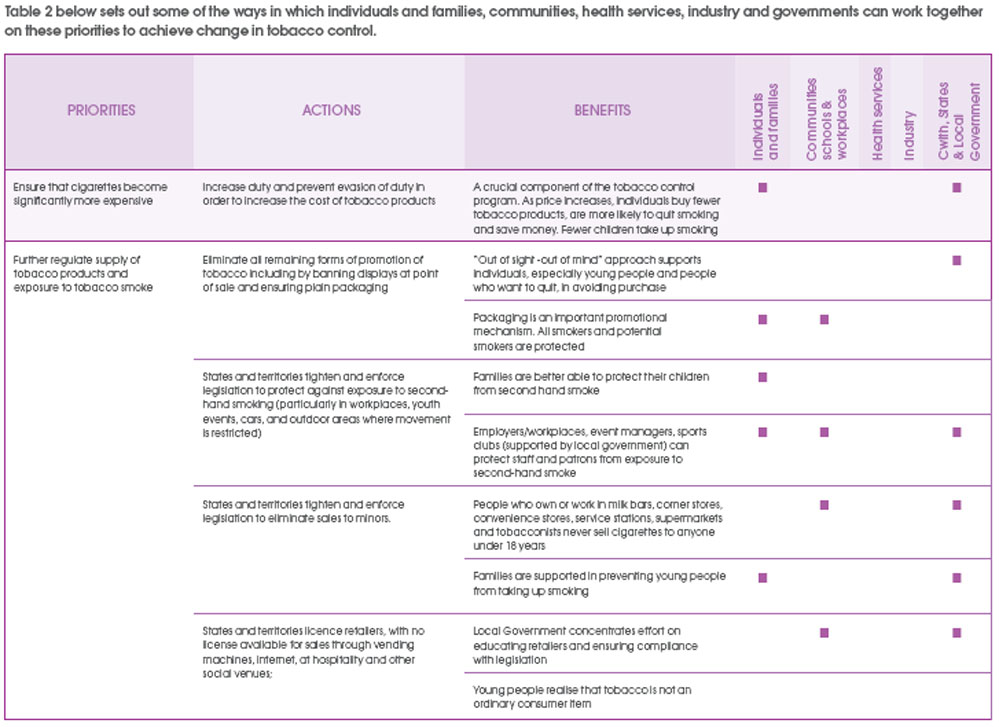
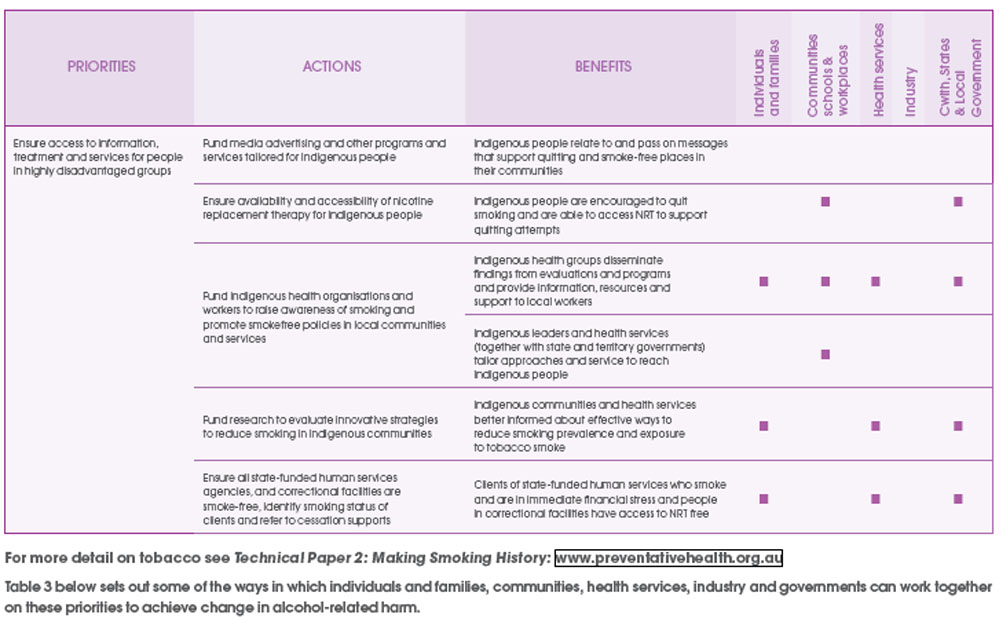
For more detail on tobacco see Technical Paper 2: Making Smoking History: www.Preventivehealth.org.au
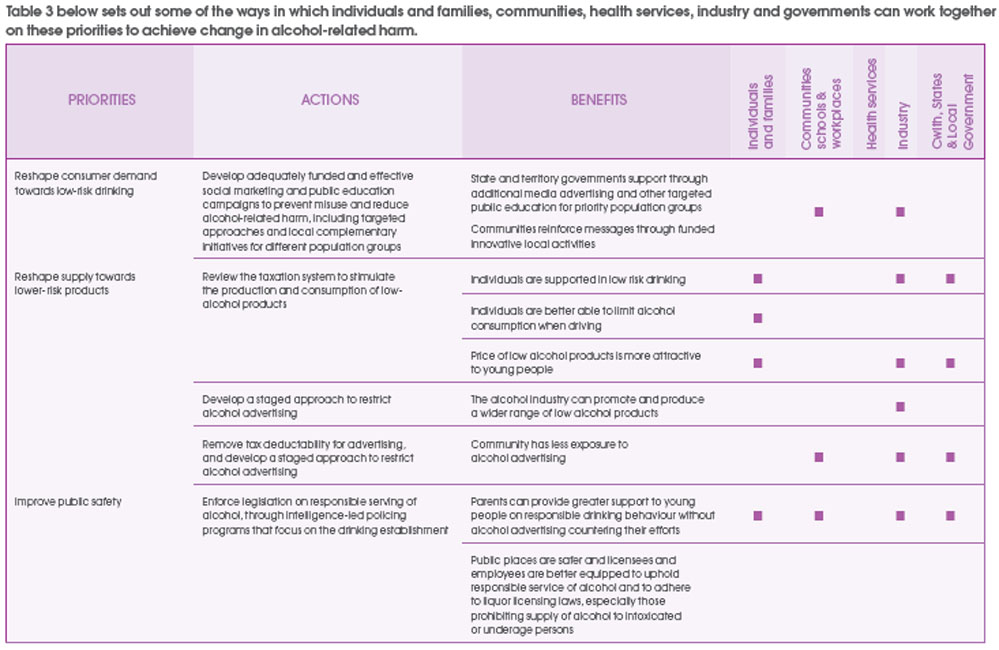
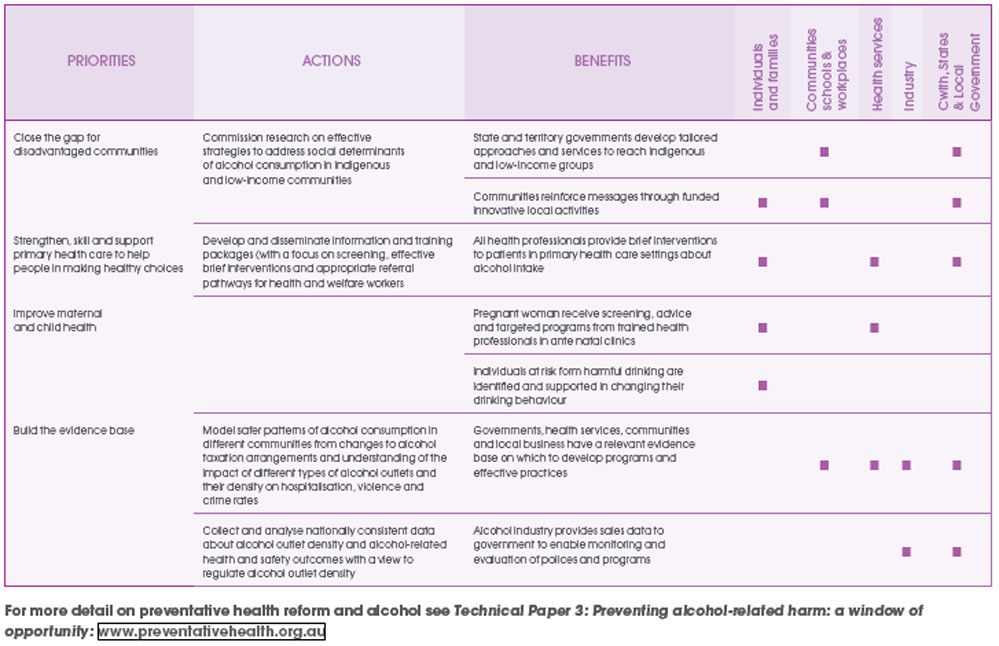
QUESTIONS
There is clear and unequivocal evidence that two actions by government will decrease the number of Australians who die early because they smoke:
-
increasing the price of tobacco products
-
sustained, well-funded, hard-hitting public education campaigns
-
Do you support our government taking the following actions, which in combination could halve smoking rates?
-
progressively increasing the tax on tobacco products to the levels in places such as Ireland, Scandinavia and the UK, and reaching $20 for a packet of 30?
-
investing $40–50m a year in public education – less than 1% of revenue from tobacco tax
-
If you do not support these actions and investment, or have other suggestions, what would you propose we do as a nation to halt the toll of early deaths and disease caused by smoking?
-
Should we prohibit all remaining forms of promotion of tobacco products and mandate plain packaging?
-
Should we move by 2020 to a system where cigarettes are sold only through a limited number of specially licensed outlets?
-
What more can we do to protect children and adults from exposure to second-hand smoke?
4. The case for prevention: alcohol
2020 target: reduce the prevalence of harmful drinking for all Australians by 30%
4.1 The current situation
Alcohol plays many roles in society – as a relaxant, as an accompaniment to socialising and celebration, as a source of employment and exports, and as a generator of tax revenue. It is intrinsically part of Australian culture.
The majority of Australians who regularly drink do so in moderation. Around three-quarters (72.6%) of Australians drink below levels that would incur long-term risk of harm. However, the short-term consumption of alcohol at harmful levels, while only occasional, is a prominent feature of Australia’s drinking culture. One in five Australians (20.4%) drink at short-term risky/high risk levels at least once a month. This equates to more than 42 million occasions of binge drinking in Australia each year. While these drinking patterns have not changed markedly over the past decade, they continue to produce substantial costs to the health of Australians, and trends among young people show cause for concern.
Australia’s international reputation in action on alcohol is among the best in the world.
A recent review of alcohol policies in 30 OECD nations rated Australia as fifth overall, ranked behind Norway (1st), Poland, Iceland and Sweden.[59] Another recent comparison of alcohol policies in 18 countries reports that ‘contrary to the generally pessimistic reports about alcohol policies, the case of Australia provides cause for optimism’.[60]
Alcohol policy experts remind us that that while there are ’some significant disappointments‘, there are also ’some wonderful examples of successful Australian public policies around alcohol from the past two decades‘: drink driving legislation and enforcement, the compulsory fortification of bakers’ flour with thiamine, and liquor licensing restrictions that are working well for some Aboriginal communities.[61]
None of this should be cause for complacency.
If success is to be measured on the basis of any change in rates of overall per capita drinking, and of adult binge drinking and outcomes such as alcohol-related deaths, hospitalisations and crime, these strategies alone are not enough. It is not only public health experts who are concerned about the harmful use of alcohol.
The general community is also worried about alcohol’s adverse health and social effects.
A recent survey of Australians showed that 84% of people are concerned about the impact of alcohol on the community and that they consider intoxication to be unacceptable.[62]
There is an urgent need to improve public safety by curbing rising levels of intoxication, reducing alcohol-fuelled violent and disruptive behaviour on the street and in the home, stepping up efforts to further reduce drink driving, and ensuring that the abuse and neglect of children through alcohol consumption is addressed.
Equally important is the need for strong enforcement of current laws and practices that prevent the harmful use of alcohol.
Current snap shot
83% of Australians are drinkers, and 1.4 million Australians consume alcohol on a daily basis. Overall per capita consumption of alcohol in Australia is high by world standards, with the country currently ranked within the top 30 highest alcohol-consuming nations, out of a total of 180 countries (WHO 2008)
Consumption accounts for 3.2% of the total burden of disease and injury in Australia: 4.9% in males and 1.6% in females[25]
The annual tangible net cost to the Australian community from harmful drinking is estimated to be almost $11 billion[63]
Much of this cost is borne outside the health system. One of the major tangible costs is lost productivity in the workplace ($3.5 billion). An estimated 689,000 Australians attend work under the influence of alcohol each year[63]
Other costs outside the health system include the costs of road accidents ($2.2 billion), costs of crime ($1.6 billion), and lost productivity in the home ($1.5 billion)
It is also estimated that alcohol is responsible for insurance costs totalling $14 million a year
The negative impacts of harmful consumption of alcohol by individuals on those around them is felt regularly by many Australians: 13.1% of Australians report being ‘put in fear’ by a person under the influence of alcohol, and 25.4% report being subjected to alcohol related verbal abuse[64]
The impact of drinking on children, by their parents and/or other adults, is a particular concern: 13% of Australian children aged two years or less are exposed to an adult who is a regular binge drinker.[65] It has been estimated that 31% of parents involved in substantiated cases of child abuse or neglect experience significant problems with alcohol use[66]
4.2 Patterns of drinking
Patterns of drinking show areas of high risk throughout life.
Overall, Australian males are more likely than females to drink at short-term risky/high-risk levels on regular (at least once a month) occasions (17% of females compared to 23% of males). However, among teenagers, females are more likely than males to regularly drink at levels of risky/high-risk of harm in the short term (28% of female teenagers compared to 24% of male teenagers). Victorian data show a worsening of the problem. The prevalence of risky drinking among 16-17 year old secondary school students in Victoria has risen from 15% in 1984 to 23% in 2005. [76]
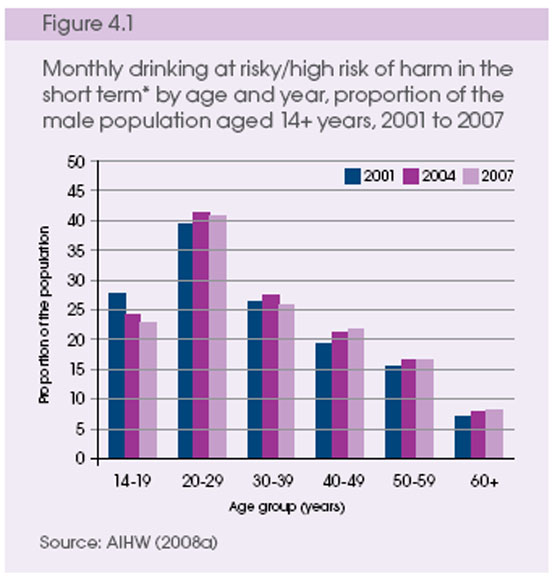 (*Risky/high-risk drinking in the short term =seven or more standard drinks on any one day for males; five or more standard drinks on any one day for females) |
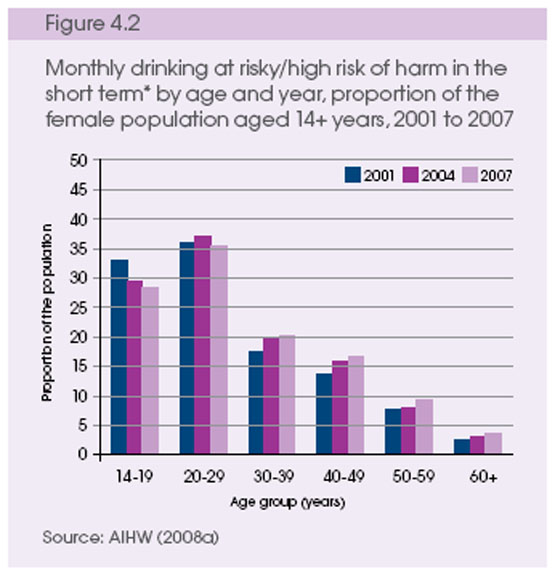 |
Between 2001 and 2007 there were only slight changes in the prevalence of drinking at risky/high risk of harm in the short term across the age groups.[4]
Among Australian teenagers in 2007, the prevalence of drinking at levels for long-term risk of harm was considerably higher among females (10%) than among males (7%).[4]
Older drinkers are also cause for concern. As the Australian population ages, heavy drinkers currently aged in their 40s and 50s are likely to present significant public health challenges by 2020 unless they reduce their alcohol consumption.
Harmful consumption of alcohol occurs in a range of different settings, and alcohol is sometimes consumed in combination with other drugs, including illicit and prescription drugs. It is also sometimes used as a substitute for other drugs.
The effects of alcohol consumption go beyond diseases, accidents and injuries to a range of adverse social consequences, both for the drinker and for others in the community. These consequences include harm to family members (including children) and to friends and workmates, as well as to bystanders and strangers. Alcohol-related disturbance and assault ranges from acts of vandalism, offensive behaviour and disruption to far more serious antisocial behaviour, which can result in violence or injury to others.[67] It is not surprising that much of the time and resources of policing in Australia are related to incidents involving alcohol.
Harmful alcohol consumption impacts significantly across a range of other areas, such as workforce productivity, healthcare services such as hospitals and ambulances, road accidents, law enforcement, property damage and insurance administration.
4.3 High-risk groups
There are variations in alcohol consumption across Australia and different impacts on specific high-risk population groups. There is geographic variation in the levels and patterns of alcohol consumption across Australia, with per capita alcohol consumption varying significantly between urban and rural areas and between Australian states and territories. For instance, the prevalence of drinking at short-term risky/high-risk levels at least monthly is 18.7% New South Wales, 19.4% in Victoria and 28.4% in the Northern Territory.
Indigenous Australians are about twice as likely to abstain from alcohol as non-Indigenous Australians, but those who do drink are up to six times more likely to drink at high-risk levels than-Indigenous people.[68]
Childhood and adolescence are critical times for brain development, and the brain is more sensitive to alcohol-induced damage during these times.[67]
Initiation of alcohol use at a young age may increase the likelihood of negative physical and mental health conditions, social problems and alcohol dependence. Regular drinking in adolescence is an important risk factor for the development of dependent or risky patterns of use in young adulthood.
Drinking within families is an important consideration. Depending on the circumstances, it can be either a positive or negative influence on the drinking behaviour of young people. A recent Australian study estimates that 13.2% or 451,621 children aged 12 years or less are at risk of exposure to binge drinking in their home by at least one adult.[65]
Drinking contributes to the three leading causes of death among adolescents – unintentional injuries, homicide and suicide – along with risk taking behaviour, unsafe sex choices, sexual coercion and alcohol overdose.[67]
Maternal drinking can result in a spectrum of harms to the unborn child, including fetal alcohol syndrome. Recent data show that 59% of Australian women drank alcohol at some time in their pregnancy and that 14% reported drinking five or more drinks in a sitting in the three months prior to pregnancy. However many women elect to abstain from alcohol some time during pregnancy – 58% during the first and second trimesters and 54% in the third trimester.[67] Although the risks from low-level drinking (such as one or two drinks per week) during pregnancy are likely to be low, a ‘noeffect’ level has not been established, and limitations in the available evidence make it impossible to set a ‘safe’ or ‘no-risk’ drinking level for women to follow in order to avoid causing harm to their unborn baby.
Other high-risk population groups whose misuse of alcohol requires specific considerations include people who have a mental health condition, people who have multiple health issues (for example, drug dependence, general poor health) and certain occupational groups.
4.4 Benefits of reform
Strong Preventive measures implemented now have the potential to reduce problems in the future. The results will most likely take a generation to be realised and they require a long-term effort. Cultural change is not instant – it involves steps along a continuum, as the tobacco experience has proven.
Reducing the prevalence of harmful consumption of alcohol is important at all life stages, as different risks emerge for different age groups. At a young age, regular drinking is a significant risk factor for the development of harmful drinking and alcohol problems in young adulthood and in later life.[67] Preventive measures that delay the uptake of drinking by young people as late as possible are critical in reducing the likelihood of drinking problems in the longer term.
If we act now , by 2020:
A 48% reduction in alcohol-attributable deaths could be achieved
People of all ages and backgrounds will feel safer in public places at night, especially at weekends in our major cities
Low-alcohol products will increase in availability and popularity
Local communities will have a greater say in the availability and management of alcohol in their local area
Commercial activity in city centres, particularly at night, will become more diverse and prosperous
Policing of alcohol problems will be proactive and targeted to situations where enforcement is most needed
Alcohol-caused road injuries and deaths will decline and rates of drink driving reach record lows
People will be more in control of their drinking and take steps to change individual drinking habits and to improve their overall health
Accident and emergency departments in hospitals will be less burdened by alcohol problems and better able to attend to people with other health problems
Australia’s productivity will increase, with reduced workplace absenteeism n There will be less drunken behaviour on the street and
Enormous reductions in the social costs of alcohol-related harm could be realised from policy measures such as higher alcohol taxation ($5940 million), brief interventions ($5830 million), partial advertising and marketing controls ($2450 million), and greater enforcement of drink drive laws ($940 million)
Source: Collins and Lapsley 2008: The avoidable costs of alcohol abuse in Australia[63]
4.5 Challenges
Challenges facing prevention efforts for alcohol include:
Complex social forces influence drinking behaviour
Australia’s drinking cultures are driven by a complex mix of powerful social forces. These include habits, customs, images and norms, and other interlocking and equally powerful forces relating to the social, economic and physical availability of alcohol, such as promotion and marketing, age restrictions, price, outlets, hours of access and service practices.[69]
Divided Commonwealth and state responsibilities an d complexity in achieving coordinated action
The policy levers that most influence the access to and price of alcohol in contemporary Australia are the alcohol taxation system (a Commonwealth responsibility) and liquor licensing systems (state and territory responsibility). Evidence from Australian and international research literature shows that economic availability (price) and physical availability (access) of alcohol within communities are two of the key determinants of harmful use of alcohol. In simple terms, when prices reduce or when access increases, consumption increases, but when prices increase or access decreases, consumption reduces.
Disparities in taxation In Australia, different taxes are applied to different products (beer, wine and spirits) reflecting the history of alcohol consumption in Australia, the status of various alcohol products and changing powers of taxation between the Commonwealth and states and territories.
These different taxation arrangements influence the prices of different categories of alcohol products unevenly, often in ways that do not promote low-risk consumption (see Figure 4.3).

Growth in alcohol availability
While not completely deregulated, liquor licensing laws and regulations in most jurisdictions have been significantly relaxed over the past decade, generally coinciding with the required reviews under the National Competition Policy. One of the effects of this has been a proliferation in the number of new licensed premises in some jurisdictions (see Figure 4.4). Along with an increase in the total number of licensed premises, there has been an increase in the numbers of premises with extended trading hours, the numbers of licences to sell packaged liquor (i.e. take away) and over time an increased concentration of licences held by just a few business.
Diversity and coordination
Future efforts to prevent harm from alcohol use will require integrated and coordinated arrangements. These arrangements will span all levels of government and fields of interest (health, law enforcement, road safety, finance and taxation), as well as non-government organisations, business and industry sectors.
Self-regulation of advertising
Regulation of alcohol advertising in Australia is subject to industry self-regulation, known as the Alcohol Beverages Advertising Code (ABAC) Scheme. The scheme is funded and administered entirely by the alcohol industry, with limited Commonwealth and state and territory government representation on the ABAC Committee, and does not cover all forms of alcohol promotion.
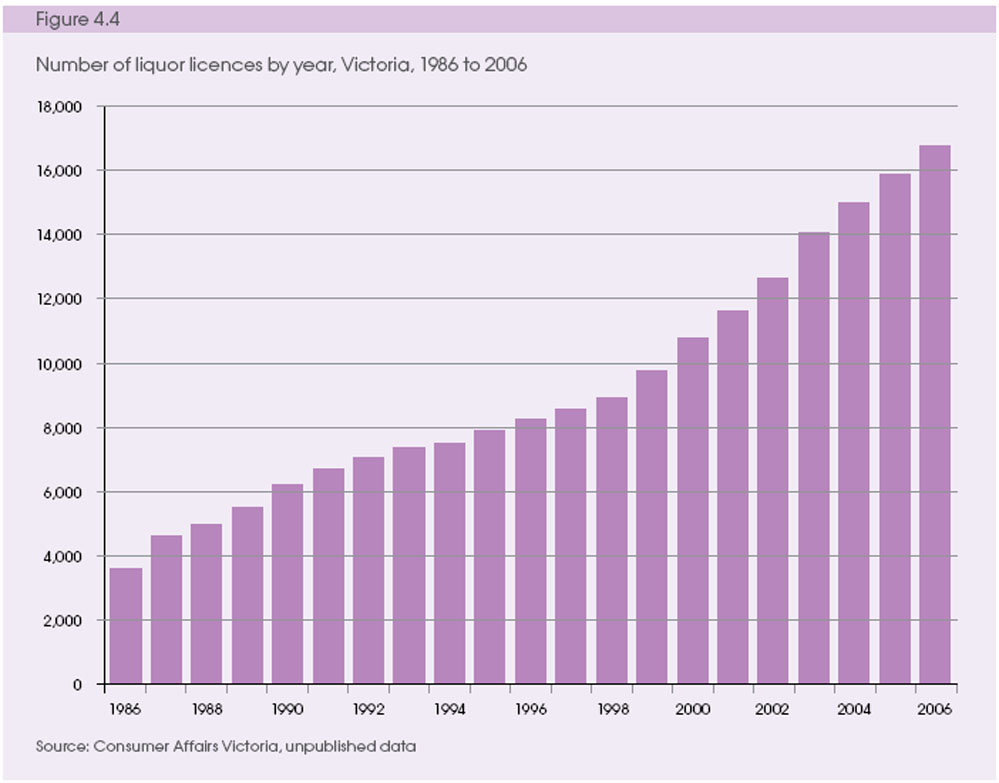
Addressing the cultural place of alcohol
A strong cultural acceptance of alcohol consumption exists in Australian society. Recent Australian research for the development of a national alcohol social marketing initiative reports, ‘
the challenge for communication is that intoxication is closely linked to alcohol per se. When we simply asked participants about their earliest memories in relation to alcohol there was an overwhelming tendency to leap to their first drunk experience. Further, these experiences were recalled with a sense of pride and nostalgia, even though the stories inevitably involved some embarrassment’.[70]
Collection of standardised data
The collection of data on alcohol sales by all state and territory governments at an outlet level is imperative. Collection will enable the analysis of changing patterns and trends in drinking and the effects of new and different types of alcohol outlets on alcohol consumption. It is also needed for the evaluation of the effects of alcohol policy measures on alcohol consumption and the rates of alcohol problems over time and in different communities.
4.6 Future outlook
The prevalence of harmful drinking and the incidence of alcohol-related harm in Australia are already at levels that cause significant social and economic costs to the community – costs that are preventable.
Current projections of the leading causes of disease burden to 2030 predict that there will be no improvement.
Based on current trends:
Young women will continue to overtake young men in the prevalence of binge drinking
Night time economies, especially in our major cities, will demand significant resources to manage alcohol related anti-social behaviour, violence and crime
Police services and hospital emergency departments will require significantly more resources to attend to alcohol-related issues, marginalising other social and health issues
Young people will increasingly be targeted through planned and sophisticated multimedia-based alcohol advertising
There will be a lack of low-alcohol beverage options available, with limited incentives to provide anything other than higher strength options
Alcohol will be available in a wide range of locations, making it hard to restrict access to alcohol and impossible to enforce liquor licensing laws
Health inequalities between Indigenous and non-Indigenous Australians, and between particular geographic areas of Australia, will be further widened
4.7 Priorities for action
Reducing the harmful consumption of alcohol requires a long-term commitment. There are many lessons to be learnt from the successes to date with tobacco control, including the phasing in of prevention strategies, and efforts to increase community understanding and shift social norms.
Internationally, experts agree that an effective strategy consists of a comprehensive approach including:
regulation of alcohol availability
enforcement of liquor laws
marketing and accessibility
raising awareness of the harmful effects of alcohol on individuals and society
implementing brief interventions against the harmful use of alcohol
improving health outcomes for Indigenous people
There is also agreement that an effective strategy needs to deal with under-age drinking, the harmful use of alcohol during pregnancy, and driving or operating machinery while under the influence of alcohol.[5]
In the first instance, the major imperatives for Australia are to:
Reshape consumer demand towards safer drinking through:
Managing both physical availability (access) and economic availability (price). The high accessibility of alcohol – in terms of outlet opening hours, density of alcohol outlets and discounting of alcohol products – is an issue in many Australian communities.
Addressing the cultural place of alcohol.
Social marketing and public education are required, and will be more effective if the marketing of alcoholic beverages is restricted, including curbing advertising and sponsorship of cultural and sporting events.
Reshape supply towards lower-risk products through:
Changes to the current taxation regime that stimulate the production and consumption of low-alcohol products.
Improved enforcement of current legislative and regulatory measures (such as Responsible Serving of Alcohol or bans on serving intoxicated persons and minors, or continuing to lower blood alcohol content in drink-driving laws).
Strengthen, skill and support primary health care to help people in making healthy choices:
Supporting brief interventions as part of routine practice by trusted health professionals and other health workers in primary healthcare settings can assist changes in drinking behaviour and attitudes to alcohol consumption.
Close the gap for disadvantaged communities
There is a need for tailored approaches and services to reach Indigenous and other disadvantaged groups.
Improve the evaluation of interventions through:
Monitoring and evaluation of regulatory measures and other programs to underpin the further evolution of prevention strategies directed at inappropriate alcohol consumption.
Developing effective models of safer patterns of alcohol consumption in different communities through changes to alcohol taxation arrangements, and an understanding of the impact of different types of alcohol outlets and their density on hospitalisation, violence and crime rates.
Recent reviews of available research evidence show that interventions targeting the whole population generally have higher effectiveness ratings and are cheaper to implement and maintain (on average) than those targeting high-risk groups.[71] In general, on the basis of experience thus far (and recognising that some other interventions have not been fully implemented and evaluated), the types of interventions that are considered most effective according to the ratings are, in order:
regulating physical availability
taxation and pricing
drink driving counter-measures
treatment and early intervention
Other areas that have very promising potential for effectiveness include:
altering the drinking context
regulating promotion
well-funded, sustained public education
There has not been enough experience to date for programs in these areas to be rated, although experience from tobacco in regulating promotion and public education is very encouraging.
High priority should be given to enforcing and extending existing legislation and regulation, coupled with public education and social marketing. The combination of these strategies has proven highly successful in tobacco control and the control of drink driving. In addition, innovative and intelligence-led approaches to law enforcement (for example, the use of information about the last place of alcohol consumption prior to an offence in order to pinpoint establishments not implementing responsible serving of alcohol) can be widely adopted.
New policy measures should also be considered. The current Treasury review of Australia’s taxation system[72] provides an opportunity to review and reform flaws in the current alcohol taxation system, especially the ways in which the current taxation system does not treat all alcohol types equally, and does not adequately tax alcohol to compensate for the negative impacts it produces.
The review should consider alternative models of alcohol taxation for Australia by utilising key data sets on consumption and technical expertise to review the current alcohol taxation system, best practice models, means of regulating minimum price and the likely effects of different models on public health.
QUESTIONS
-
Do you support a focus on the suggested priorities?
-
If you do not support these actions, or have other suggestions, what would you propose we do as a nation to halt the toll of early deaths and disease caused through alcohol-related harm?
-
What are the most important issues that can engage support from individuals, communities, industry and governments and drive cultural change?
-
What prevention strategies work best for high-risk groups, particularly among young people and in Indigenous communities?
5. Supporting prevention
5.1 Common aspects across obesity, tobacco and alcohol
A comprehensive package of reform will require action on each of the following, both separately and in combination.
Access and affordability
The price of tobacco and alcohol products and their availability are two of the crucial factors in reducing smoking and alcohol consumption. Similarly, price and availability should not be barriers to healthy eating and physical activity. This requires healthy foods to be cheaper and more accessible, and physical activity options to be easy and cheap for individuals to undertake. Price and availability are generally changed through legislation, taxation and regulation.
Product marketing
Advertising, packaging, labelling and promotion of products are standard ways in which all manufacturers and retailers increase sales and drive up income. The more attractive the product, the greater the public interest. Reducing, curbing or (as with tobacco) eliminating these aspects of product marketing makes unhealthy products less attractive to the public in general and to children in particular.
Making unhealthy products less attractive will require different strategies in each of the three areas. For example, tobacco control requires the elimination of all forms of advertising and promotion. Action on alcohol and obesity will need effective controls, working with the food and beverage industries to ensure constraints on inappropriate marketing and to ensure the availability and promotion of healthy food and beverage options.
Public education
Experience from tobacco control, road safety, HIV prevention and other areas demonstrates that well-planned, appropriately funded and sustained public education campaigns are a vital and effective component of prevention programs, and will be required over the coming years for obesity, tobacco and alcohol. Such campaigns also require investment at a level that enables targeting of different population subgroups, and locally based supporting strategies where appropriate.
Community engagement
Without the goodwill and interest of Australian communities, reform will be difficult to achieve. If individuals are to make healthy choices they require support and reinforcement from their families and communities that these are the right choices.
Settings for action
School communities, childcare and maternal health programs, workplaces, sports venues and local government settings provide useful designated environments in which to undertake a combination of interventions. To be successful, programs delivered in all settings should adopt an integrated approach incorporating the three priority areas of obesity, tobacco and alcohol.
Mix of universal and targeted action
Shifting population norms requires small changes from everyone, but additional and different efforts are often needed for disadvantaged populations. Addressing health risks from obesity, tobacco and alcohol are important ways to help close the health gap. In order to target health inequalities, such as those in disadvantaged populations and settings, programs should be appropriate and meet the needs of the target group, and encourage and assist individuals to take action within their community.
A lifelong framework for action Policy reform and strategies for action require a lifelong approach. While emphasis is placed on pregnant women and early childhood, there are other critical times in life that are also important if momentum is to be maintained.[73] For example, there should be a focus on groups such as toddlers, school-aged children, first-time parents and older Australians.
Skilled workforce
A skilled and motivated workforce, especially in the public health and primary healthcare sectors, will be essential to support delivery of health promotion and Preventive health measures across the community. For example, bringing primary healthcare providers such as general practitioners, community pharmacists, nurses, psychologists and other allied health professionals together for community-based training and support provides a way of ensuring a comprehensive and well-coordinated approach to Preventive health care.
Development, dissemination and training to ensure the uptake of evidence-based guidelines is important, as is curriculum development to educate future generations of health professionals and community workers.
5.2 Support structures
The recent history of public health in Australia shows that Preventive efforts have been most effective when effective supports have been put in place. Supports include:
Leadership and coordination
Research to build the evidence base
Capability in surveillance, program evaluation, social marketing, legislation and regulation, and community mobilisation
Targeted and sustained intervention strategies
Sustainable financing and incentive-based funding
An appropriately skilled workforce
Integrated evidence, policy and practice
Partnerships and collaboration
Community engagement
Inadequately funded or single, short-term and ad hoc projects and programs are unlikely to succeed and may be counter-productive, as they give rise to an argument that ’prevention doesn’t work’, when in fact real and sustained prevention has not been tried. Separate infrastructure investments for efforts targeting each risk factor will be costly. A robust prevention support system is required, including mechanisms for the coordination of strategies that cut across all the issues. The strategies recommended above require interventions in schools, primary health care, workplaces and other settings, regardless of the specific health risk. The planning and evaluation of these efforts will require a well-coordinated surveillance system that can track health conditions, risk factors, social and demographic factors, and exposures. All these activities will also require the concerted efforts of a well-trained workforce.
5.3 Major imperatives to strengthen support systems
LEADERSHIP AND COORDINATION
It is important to ensure leadership and coordination through the establishment of a National Prevention Agency.[74]
A National Prevention Agency (NPA) is long overdue. Such an organisation would take the leadership role in ensuring the implementation and support of prevention programs nationally.
The NPA could support the coordination of partnerships and interventions, ensuring the relevance and quality of workforce training activities, social marketing, public education and the monitoring and evaluation of interventions.
The NPA would consist of a relatively small group of credible leaders in prevention, with a track record and capacity to ‘make things happen’ for Preventive health reform.
By bringing together expertise across relevant areas, a national agency would provide leadership for the implementation of the National Preventive Health Strategy and build prevention systems with strong capabilities in the following areas:
Ensure the delivery of a minimum set of evidence-based, prevention programs that are accessible to all Australians.
Allocate funding to its partners for activities that deliver the National Preventive Health Strategy’s goals and targets.
Contribute to closing the gaps between Indigenous Australians and the rest of the population in association with other relevant organisations such as the National Indigenous Health Equity Council.
Engage key leaders and build new partnerships across federal, state and territory governments, national agencies, professional associations, local government, peak community groups, NGOs, the private sector, the philanthropic sector and academe.
Support the integration of research, policies and strategies for illness prevention/health promotion across sectors and settings within and beyond health care.
Commission and promote the uptake of new monitoring, evaluation and surveillance models for illness prevention.
Promote the benefits of illness prevention/ health promotion as measured by these new evaluation models.
Serve as an authoritative source of information on evidence, policy and practice.
Develop the evidence base on prevention through the design, implementation and evaluation of large-scale programs to improve the health and wellbeing of the population, or population sub-groups, by testing innovative strategies, programs and policies for illness prevention/health promotion.
Ensure the development of the necessary national workforce for illness prevention/health promotion, working with and through relevant national, state and local agencies to build capability in:
surveillance, prevention research, evaluation, economic impact research and modelling
social marketing and public education
community development
legislation, regulation, economics and taxation
leadership and management.
The agency’s approach would support the following groups in the workforce:
People working in prevention including health promotion practitioners and public health researchers.
Others working in the healthcare system, including general practitioners, allied health professionals, specialists, Aboriginal health workers and health service managers.
Those working in other sectors that have a role in prevention; for example, in local government, police and justice, education, sport and recreation, urban planning, transport and agriculture.
Surveillance
Establish a comprehensive national surveillance system, working in partnership with AIHW and ABS. This would focus on the behavioural, environmental and biomedical risk factors for chronic disease (including factors such as food availability and food composition) to track and report on performance and outcomes, including the impact on health inequalities. (For example, expanding the national nutrition and physical activity survey program through the inclusion of biomedical data.)
Prevention research and evaluation
Partnerships with the National Medical and Research Council (NHMRC) and the Australian Research Council (ARC) and other state based research funding organisations (such as health promotion foundations) will be important to ensure a coordinated investment approach for research and evaluation. Research would include an understanding of social determinants of health behaviour, the modelling of health impact of policy options and the evaluation of programs.
Social marketing and public education
It will be important to commission research and development of targeted social marketing and public education campaigns. This mechanism would also be used to coordinate national media advertising with local program delivery, and to evaluate their effectiveness.
Tobacco control has shown the effectiveness of these measures.Incentive-based funding
A prevention benefit item included in the Medical Benefits Scheme would support delivery in primary care practices of brief interventions and follow-up (whether they were directed to tobacco, alcohol, obesity or other relevant chronic disease risk factors).
The structure of the item could be a small add-on to standard consultations in primary care practices when the intervention is delivered and as a stand-alone item at follow-up. Such a structure could help narrow the opportunities for inappropriate use and practice, as well as help improve the evidence base.
Supporting primary health practices to enhance their role in prevention
Primary health care is a fundamental part of Preventive health. This is seen in many areas, including immunisations, screening for cancers and, as we have seen earlier, brief interventions to discuss and advise on smoking and alcohol use. Three approaches are suggested:
There is increasing consensus around the need to define the population that a practice is working with and for. This would have to start with enrolling or registering patients in a practice.
Adequate incentives at the practice level (for example, Practice Incentive Payments) or at individual practitioner level (for example, Medicare Benefits Schedule item number) must be provided. Given that brief interventions and the use and promotion of life scripts can be very adequately done by practice nurses, this incentive would be better placed at the practice level.
A system of accountability and reporting is needed to complement the incentive payment scheme.
QUESTIONS
Do you support the development of a National Prevention Agency to lead and guide coordinated action for prevention?
Is the suggested approach adequate? If not, or if you have other suggestions, what else should be considered?
6. Choosing performance indicators
Australia will need to know the results of the approaches implemented now and into the future. It will be essential to monitor progress at three levels:
Health status and outcomes
Determinants of health
Health (and other) systems performance
Identification of progress needs a performance framework that shows:
How well in the longer term we are achieving health status and outcomes (for example, deaths attributable to obesity and overweight, to tobacco and to alcohol)
How well in the longer term we are addressing obesity, tobacco and alcohol in relation to the determinants of health (for example, measure the proportion of adults who are overweight or obese, daily smokers and at risk of long-term harm from alcohol)
Whether there are improvements in Indigenous health status
These kinds of measures are affected by many factors, and changes cannot easily be attributed to specific programs. It can also take many years before an impact on personal behaviours and health outcomes is achieved. To balance this longer term measurement with some short-term measures, indicators will also need to be set to measure
health and related systems performance. These measures are more closely related to the specific priority interventions and in some cases will be most sensitive in the short term to their effective introduction (for example, public education campaigns). Some interventions may be difficult to measure using current information systems (for example, alcohol outlet density) and will require the development of new systems. The proposed performance indicators in each category are tabled below.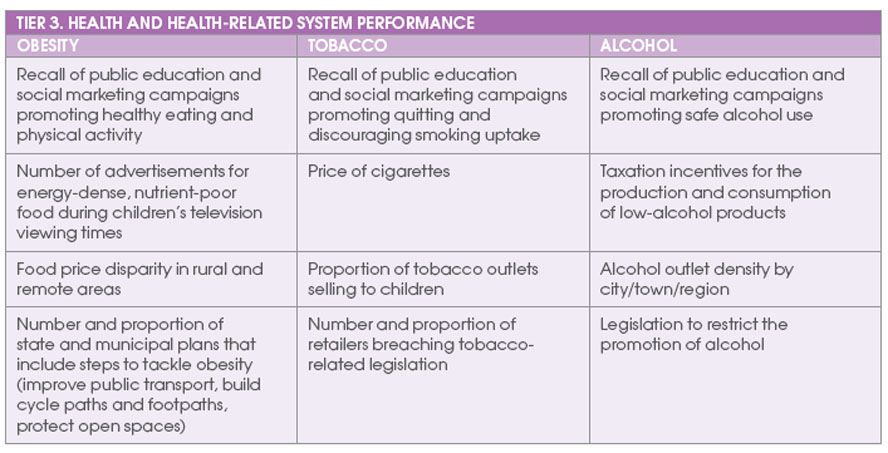
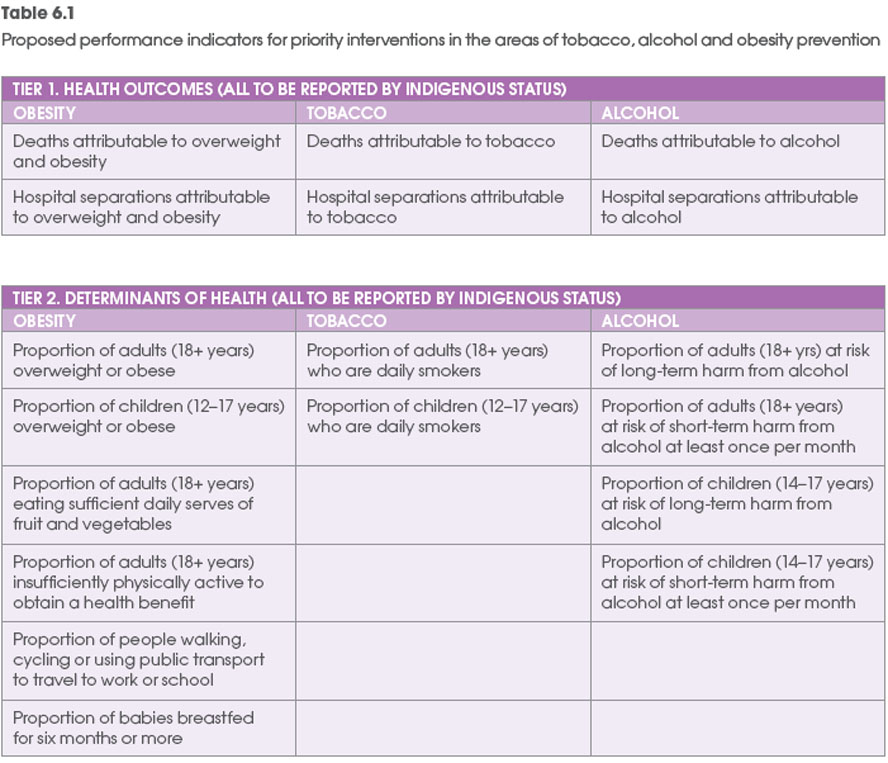
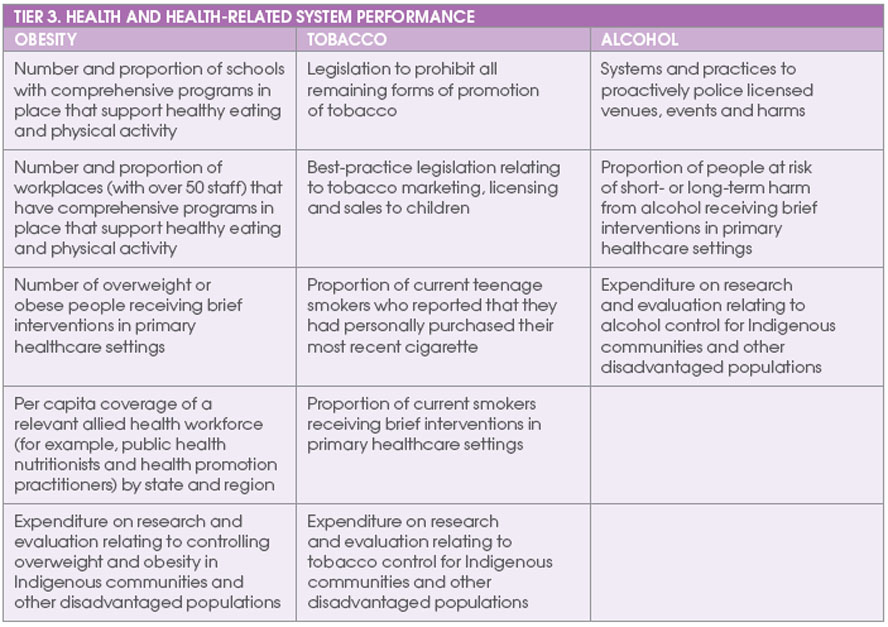
Enabling infrastructure
-
Use of data generated from surveillance system focused on the behavioural, environmental and biomedical risk factors for chronic disease
-
Number of staff working in appropriate public health activities
-
Places for community-based training for primary healthcare (and other) workforce
-
Expenditure on research and development of targeted social marketing and public education efforts and to coordinate national media advertising with local program delivery
-
Uptake of Medicare Benefits Schedule prevention benefit item
-
Expenditure on prevention research, including understanding of social determinants of health behaviour, modelling of health impact of policy options and evaluation of programs
-
Satisfaction of health and other groups (including community organisations, private sector, and other interests) with engagement with government health agencies
6.2 Monitoring the indicators
Health outcomes indicators can be monitored using existing data collections. In most cases these indicators are already routinely reported by the Australian Institute of Health and Welfare in
Australia’s Health and related reports.Mortality and hospital separations attributable to overweight and obesity are exceptions; however, the data needed to estimate these are readily available.
Determinants of health can be monitored using existing data collections. Measured data on height and weight for adults and children were collected in the 2007–08
National Health Survey and the 2007 national Kids Eat, Kids Play survey. Data relating to active transport are less readily available. The National Health Survey collects data only on whether people walked for transport; however, state-based telephone surveys have collected more detailed information on mode of transport to work and school.The addition of five-yearly national health studies would enhance our monitoring of prevention polices, activities and outcomes.
6.3 Setting targets
Detailed work will be required in order to set targets for our proposed indicators. Targets should be set for the indicators in all three tiers.
However, if, under the Council of Australian Governments (COAG) system, payments are to be tied to performance against targets, we suggest that indicators for this purpose be selected from the health and related systems performance tier. More work would be needed to refine many of the indicators in this tier for this purpose.
In many cases, targets would need to be state or territory specific, recognising differences in the current population prevalence of health risk factors, population profiles (for example, socioeconomic status, Indigenous population) and the challenges in introducing interventions in different settings (urban/rural/remote).
6.4 Governance and performance monitoring
COAG is currently developing a system of National Partnership Payments (NPPs) aimed at providing incentive payments to states and territories for reforms, or for specific and agreed joint projects, within a new performance and assessment framework. To receive funding, states and territories must deliver ‘nationally significant economic and social reforms’. Payments are structured, with a fixed duration, and offer up-front facilitative/reward payments for achievement against performance benchmarks.
There are many different ways in which funding incentives can be provided. Examples of pay-for-performance incentives exist in the personal healthcare area in Australia, as well as internationally.
Incentives can be tied to global performance or to specific service items. Both rewards and penalties have been incorporated into previous Medicare agreements for hospital funding, and experience suggests that a punitive system has high transactional costs and does not encourage a transparent and collaborative approach.
A simple approach is to have a quantum of funds that is ‘at risk’ for each state and tied to the achievement of targets in that state.
For example, incentive payments could be provided for against reaching a target of reduction in smoking prevalence in the state.
A more competitive approach is to have a pool of funds with states receiving funds proportional to their performance towards joint health outcomes. For example, the additional funding available to a jurisdiction would be dependent on the reduction in smoking in that state relative to the national reduction in smoking prevalence.
Incentive payment systems, particularly those based on health outcomes, have several inherent risks:
Difficulties in attributing change to specific state reform efforts, given the need for joint action leading to joint outcomes.
Inconsistencies that arise where there are inadequate or incomparable data collection systems, which either under-report or over-report.
Overemphasis placed on particular actions to the exclusion of other important health concerns distorts the focus of work.
Higher rewards for those who start with more resources or relatively easier tasks compared to those with more complex tasks and fewer funds.
Slow rates of change in health indicators, along with the many socio-economic determinants that can influence health outcomes.
The payment system will need to be underpinned by:
A sound monitoring system – including both the adequacy of data and indicators, and an appropriate process of review
Agreement about the appropriate points in time for assessment
Mechanisms for stimulating improvements should performance be disappointing
Given that the data systems related to prevention activities need further development, a phased approach may be necessary, with indicators modified or incorporated as the NPP system evolves.
6.5 The monitoring system
A good monitoring system is essential for Preventive health reform to work and to ensure that Commonwealth, state and territory activity is regularly reviewed. It can also play a critical role to assist learning, as well as assessing performance. In addition, beyond the compilation of data, there are several important principles:
Relevance
Link with governance processes including other reporting and monitoring systems
Link with and contribute to health program improvement
Analyse and interpret to address key policy concerns and potential for action Data collection
Build on existing systems for data collection (including surveys and administrative data)
Work on improving specificity of national reporting and harmonisation of jurisdictional data systems (through common data definitions and standards)
Build on indicators proposed through key international consensus and reporting frameworks, using proxy indicators when collecting additional data is not feasible
Have a designated national focal point, located within an appropriate setting, with accountability for data collection and dissemination
Reporting
Have a regular reporting time frame
Offer sufficient specificity (including location, sex, ethnicity, age and socio economic status)
Provide quantitative and qualitative indicators and analyses, which ensure that local contexts are explicitly taken into account in the reporting system
Enable analysis and reporting of trend data on core sets of indicators n Enable analysis and reporting by appropriate groupings involving a similar population mix for comparative assessment [75]
Have a manageable set of core indicators nationally but also develop optional modules that allow for harmonisation and comparison across similar communities or regions
Have an accessible, appealing and user-friendly reporting style that engages and is useful to stakeholders
Provide annual reporting against the proposed National Preventive Health Strategy
Provide regular public reports on progress
Capacity building
Capacity building mechanisms and processes in place to train and support an enhanced understanding of meaning and action potential of the key performance indicators
Capacity building at regional and local levels
Create a continuing social process for accountability by developing mechanisms to bring together key stakeholders at both national and global levels to review and discuss action requirements arising from leading health indicators
QUESTION
Are these measurements appropriate? If not, what would you propose?
7. Towards a National Preventive Health Strategy – your views
The Preventive Health Taskforce invites your input to the next stage of development of a National Preventive Health Strategy
This discussion paper provides the first step in the development of the Strategy. We have proposed targets for three key areas of prevention - obesity, tobacco and alcohol, together with priorities and recommended policies and programs. We have also identified the support structures and measurements needed to ensure that the key priorities are met and that there is proper monitoring and evaluation.
A series of questions have been put forward in this paper. The Taskforce is keen to hear your responses and to have your input as we work towards developing the Strategy.
Throughout the paper, an emphasis is placed on working together. We invite all - individuals, community groups, government and non-government organisations and industry groups - to participate by making a submission on how we can make Australia the healthiest nation by 2020. We suggest you take the questions in this paper as a starting point, although we welcome your views on other issues.
The Taskforce will also be holding national consultations from October 2008 to February 2009
Submissions can be made by 2 January 2009 by using the form provided at the Taskforce website: http://www.Preventivehealth.org.au
Content of submissions
Your submission should include:
Name and full contact details (including email address), company name (where applicable) and designation of submitter. A form for proving this information can be found at the Taskforce website: http://www.Preventivehealth.org.au ;
Comment on areas/questions set out in the Discussion Paper;
Any other relevant information (for example any technical, economic or business information, or research-based evidence supporting the view being expressed);
Identification and discussion of any perceived omissions in the Discussion Paper or alternative approaches.
Contact Details for the Taskforce Secretariat:
Mail: Preventive Health Taskforce Secretariat
MDP 16
Department of Health and Ageing
GPO Box 9848
CANBERRA ACT 2601
Email: pht.secretariat@health.gov.au
Telephone: 02 6289 4426
Please note that the Taskforce will not provide a written response to submissions.
Publication of submissions
Unless otherwise indicated in the submission, all submissions may be published on the Preventive Health Taskforce website. If you wish any information contained in your submission to be treated as confidential, please explicitly and clearly identify that information, and outline the reasons why you consider it to be confidential. Note that general disclaimers in covering letters will not be interpreted as a specific request or taken as sufficient reason for submissions to be treated confidentially.
Please note that any request under the Freedom of Information Act 1982 for access to a document (regardless of the document’s assigned classification) in the possession of the Commonwealth will be determined in accordance with that Act.
References
1. Aboriginal and Torres Strait Islander Social Justice Commissioner and the Steering Committee for Indigenous Health Equality. Close the gap. National indigenous health equality targets. Outcomes from the National Indigenous Health Equality Summit Canberra. Sydney: Human Rights and Equal Opportunity Commission, 2008. Available from: http://www.hreoc.gov.au/social_Justice/health/targets/health_targets.pdf
2. Department of Human Services. Life expectancy at birth: Victoria 2001-2005. Melbourne: Department of Human Services, Victoria, 2007. Available from: http://www.health.vic.gov.au/healthstatus/le-01-05.htm
3. World Health Organization. Closing the Gap in a Generation. Geneva, 2008. Available from: http://whqlibdoc.who.int/hq/2008/WHO_IER_CSDH_08.1_eng.pdf
4. Australian Institute of Health and Welfare. Australia’s Health 2008. Cat No. AUS 99. Canberra: Australian Institute of Health and Welfare, 2008. Available from: http://www.aihw.gov.au/publications/index.cfm/title/10585
5. World Health Organization. Prevention and control of non-communicable diseases: implementation of the global strategy. World Health Organization, 2008. Available from: http://www.who.int/gb/ebwha/pdf_files/A61/A61_8-en.pdf
6. Holman C and Smith F. Implications of the obesity epidemic for the life expectancy of Australians. Report to the Public Health Advocacy Institute of Western Australia 2008. Available from: www.phaiwa.org.au/index.php?option=com_content&task=view&id=61&itemid=967 . Doll R, Peto R,Boreham J and Sutherland I. Mortality in relation to smoking: 50 years’ observations on male British doctors. BMJ (Clinical Research Ed.).
2004;328:1519. Available from: http://www.bmj.com/cgi/content/abstract/328/7455/1519
8. Doherty S and Roche A. Alcohol and licensed premises: best practice in policing. A monograph for police and policy makers. Adelaide: Australasian Centre for Policing Research, 2003. Available from: www.nceta.flinders.edu.au/pdf/licensed-premises/licencedpremises.pdf
9. Collins D and Lapsley H. The costs of tobacco, alcohol and illicit drug abuse to Australian society in 2004/05. P3 2625. Canberra: Department of Health and Ageing,
2008. Available from: http://www.nationaldrugstrategy.gov.au/internet/drugstrategy/publishing.nsf/Content/mono64/$File/mono64.pdf
10. Access Economics. The growing cost of obesity in 2008 :three years on. Canberra: Diabetes Australia, 2008. Available from: http://www.diabetesaustralia.com.au/PageFiles/7832/FULLREPORTGrowingCostOfObesity2008.pdf
11. d’Espaignet T et al. Trends in sudden infant death syndrome in Australia from 1980 to 2002. Forensic science, medicine, and pathology. 2008:1547-769X. Available from: http://www.springerlink.com/content/702m248283174687/
12. Abelson P and Applied Economics. Returns on Investment in Public Health. Canberra: Department of Health and Ageing, 2003.
13. Taylor R and Clements M. The contribution of the decline in tobacco smoking to reduced lung cancer mortality in Australia; The contribution of reduction in tobacco smoking to the decline in chronic obstructive pulmonary disease mortality in Australia; The contribution of changes in risk factors to the decline in coronary heart disease mortality in Australia 1968-98, in Applied Economics, Returns on Investment in Public Health: An epidemiological and economic analysis, Canberra: Department of Health and Ageing, 2003;
14. Trust for America’s Health.
Prevention for a Healthier America: INVESTMENTS IN DISEASE PREVENTION YIELD SIGNIFICANT SAVINGS, STRONGER COMMUNITIES. Trust for America’s Health, 2008. Available from: www.healthyamericans.org15. Garret L. Betrayal of Trust; The Collapse of Global Public Health. New York: Hyperion, 2000.
16. Rudd K. A future agenda for Australia. Brisbane: Australian Labor Party, 2007, Last modified June 2008 [viewed September 2008]. Available from: http://www.pm.gov.au/media/Speech/2008/speech_0329.cfm
17. Australian Institute of Health Policy Studies and VicHealth. A vision for prevention in Australia: National Prevention Summit 2008 Discussion Paper. national Prevention Summit. Park Hyatt Melbourne, 2008.
Available from: http://www.vichealth.vic.gov.au/assets/contentFiles/FINAL_discussion_paper_.pdf
18. World Health Organization. The Ottawa Charter. Geneva: World Health Organization, 1986.
19. Commission on Social Determinants of Health. Final Report Geneva: World Health Organization, 2008. Available from: http://www.who.int
20. National Health and Hospitals Reform Commission. Principles for Australia’s Health. 2008. Available from: www.nhhrc.org.au/principles
21. Cameron A, Welborn T, Zimmet P, Dunstan D, Owe, Salmon J, et al. Overweight and obesity in Australia: the 1999-2000 Australian Diabetes, Obesity and Lifestyle Study (Aus Diab). Medical Journal of Australia. 2003;178:427-32.
22. Vos T, Barker B, Stanley L and Lopez A. The burden of disease and injury in Aboriginal and Torres Strait Islander peoples 2003. Brisbane: School of Population Health, The University of Queensland, 2007. Available from: http://www.uq.edu.au/bodce/index.html?page=68411
23. Organisation for Economic Co-operation and Development (OECD). Health at a glance 2007 - OECD indicators. 4th ed. . 2007.
24. Begg S, Vos T, Barker DC, Stanley L and Lopez A. Burden of disease and injury in Australia in the new millennium: measuring health loss from diseases, injuries and risk factors. Medical Journal of Australia. 2008;188:36−40. Available from: http://www.mja.com.au/public/issues/188_01_070108/beg10596_fm.html
25. Begg S, Vos T, Barker B, Stevenson C, Stanley L and Lopez A. The burden of disease and injury in Australia 2003. PHE 82. Canberra: Australian Institute of Health and Welfare, 2007. Available from: http://www.aihw.gov.au/publications/index.cfm/title/10317
26. The Rand Organisation. Rand report. 2007, [viewed 1 September 2008]. Available from: http://www.rand.org/pubs/research_briefs/2007/RAND_RB9043-1.pdf
27. Department of Human Services (DHS). Future prevalence of overweight and obesity in Australian children and adolescents, 2005-2025. Melbourne: Victorian Government, 2008.
28. Department of Health and Ageing Population Health Strategy Unit. Overweight and obesity in Australia: overview of trends, distribution and program response. Preventive Health Taskforce, 2008.
29. Mulhivill C and Quigley R. The management of obesity and overweight. An analysis of reviews of diet, physical activity and behavioural approaches. Evidence briefing (1st ed). Health Development Agency, 2003. Available from: http://www.nice.org.uk/niceMedia/documents/obesity_evidence_briefing.pdf
30. Medibank Private. The cost of physical inactivity. What is the lack of participation in physical activity costing Australia? Medibank Private, 2007. Available from: www.medibank.com.au/Client/Documents/Pdfs/pyhsical_inactivity.pdf
31. World Health Organization. Obesity: preventing and managing the global epidemic: report of a WHO consultation. WHO Technical Report Series. Geneva: World Health Organization, 2000. Available from: http://www.who.int/bookorders/anglais/detart1.jsp?sesslan=1&codlan=1&codcol=10&codcch=894
32. Australian Institute of Health and Welfare. Obesity and workplace absenteeism among older Australians. Cat No. AUS 67. Canberra: Australian Institute of Health and Welfare, 2005. Available from: http://www.aihw.gov.au/publications/aus/bulletin31/bulletin31.pdf
33. Doll R and Hill A. Smoking and carcinoma of the lung: preliminary report. British Medical Journal. 1950;2:739–48. Available from: http://www.pubmedcentral.nih.gov/picrender.fcgi?artid=2038856&blobtype=pdf
34. Wynder E and Graham E. Tobacco smoking as a possible etiologic factor in bronchogenic carcinoma. Journal of the American Medical Association. 1950;143:329-36.
35. Jamrozik K and Le M. Tobacco’s uncounted victims. Medical Journal of Australia. 2001;174:490–1. Available from: http://www.mja.com.au/public/issues/contents174.html#21may
36. Begg S, Vos T, Barker DC, Stanley L and Lopez A. Burden of disease and injury in Australia in the new millennium: measuring health loss from diseases, injuries and risk factors. eMJA. 2007;188:36-40.
37. Winstanley M and White V. Chapter 8. Tobacco use among Aboriginal peoples and Torres Strait Islanders, in Scollo, M. and M. Winstanley, Editors, Tobacco in Australia: facts and issues, Melbourne: Quit Victoria, 2008; In press.
38. Hill D and Gray N. Patterns of tobacco smoking in Australia. Med J Aust. 1982;1:23-5. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=927253&query_hl=12&itool=pubmed_docsum
39. Hill D and Gray N. Australian patterns of smoking and related health beliefs in 1983. Community Health Stud. 1984;8:307-16. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db=pubmed&cmd=Retrieve&dopt=AbstractPlus&list_uids=6518750&query_hl=15&itool=pubmed_docsum
40. Hill D. Australian patterns of tobacco smoking in 1986. Med J Aust. 1988;149:6-10. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=search&DB=pubmed
41. Hill D, White V and Gray N. Australian patterns of tobacco smoking in 1989. Med J Aust. 1991;154:797-801. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=Search&DB=pubmed42. Hill D and White V. Australian adult smoking prevalence in 1992. Aust J Public Health. 1995;19:305-8. Available from: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=Search&DB=pubmed
43. Hill DJ, White VM and Scollo MM. Smoking behaviours of Australian adults in 1995: trends and concerns. Med J Aust. 1998;168:209-13. Available from: http://www.mja.com.au/public/issues/mar2/hill/hill.html
44. White V, Hill D, Siahpush M and Bobevski I. How has the prevalence of cigarette smoking changed among Australian adults? Trends in smoking prevalence between 1980 and 2001. Tob Control. 2003;12:ii67-ii74. Available from: http://tobaccocontrol.bmj.com/cgi/content/full/12/suppl_2/ii67
45. Australian Institute of Health and Welfare. 2001 NationalDrug Strategy Household Survey: detailed findings. AIHW cat. no. PHE 41. Drug statistics series No. 11. Canberra: AIHW 2002. Available from: http://www.aihw.gov.au/publications/index.cfm/title/8227
46. Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2004-detailed findings AIWH cat. no. PHE 66. Canberra: Australian Institute of Health and Welfare, 2005. Available from: http://www.aihw.gov.au/publications/index.cfm/title/10190
47. Australian Institute of Health and Welfare. 2007 National Drug Strategy Household Survey: first results. Drug Statistics Series, Number 20. Canberra: Australian Institute of Health and Welfare, 2008. Available from: http://www.aihw.gov.au/publications/phe/ndshs07-fr/ndshs07-fr-no-questionnaire.pdf
48. White V and Hayman J. Smoking behaviours of Australian secondary students in 2005. Canberra: Drug Strategy Branch, Australian Government Department of Health and Ageing, 2006. Available from: http://www.nationaldrugstrategy.gov.au/internet/drugstrategy/publishing.nsf/Content/mono59
49. Scollo M. Chapter 2. Trends in tobacco consumption, in Scollo, M., and Winstanley, M, Editor, Tobacco in Australia: Facts and Issues, Melbourne: The Cancer Council Victoria, 2008; In press
50. VicHealth Centre for Tobacco Control. Tobacco control: a blue chip investment in public health. Melbourne: The Cancer Council Victoria, 2003, Last modified July 2004 [viewed. Available from: http://www.vctc.org.au51. Australian Institute of Health and Welfare. Chronic diseases mortality. Canberra: Australian Institute of Health and Welfare, 2005, Last modified 23 June 2005 [viewed 12 August 2008]. Available from: http://www.aihw.gov.au/cdarf/data_pages/mortality/index.cfm
52. Scollo M. Chapter 9. Smoking and social disadvantage, in Scollo, M. and M. Winstanley, Editors, Tobacco in Australia: facts and issues, Melbourne: The Cancer Council Victoria, 2008; In press
53. Australian Bureau of Statistics. 4722.0.55.004--Tobacco Smoking-- Aboriginal and Torres Strait Islander people: A snapshot, 2004-05 Canberra: Australian Bureau of Statistics, 2007, Last modified 5 July 2007 [viewed January 2008]. Available from: http://www.abs.gov.au/AUSSTATS/abs@.nsf/productsbyCatalogue/D030A9BD9BF14B08CA25730E0021BCE1?OpenDocument
54. Gartner CE, Reported smoking inside and outside in households with and without dependent children, data from National Drug Strategy Household Survey 2004. Brisbane: University of Queensland. Unpublished data 2008.
55. Laws P, Grayso and Sullivan E. Smoking and pregnancy. AIHW Cat. No. PER 33. Sydney: AIHW National Perinatal Statistics Unit, 2006. Available from: http://www.npsu.unsw.edu.au/NPSUweb.nsf/resources/AMB_2004_2008/$file/Smoking+and+pregnancy+for+web.pdf
56. Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework 2006. Canberra. IHW 20. Canberra: Australian Institute of Health and Welfare, 2007. Available from: http://www.aihw.gov.au/publications/ihw/atsihpf06r/
57. US Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, Georgia: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004. Available from: http://www.cdc.gov/tobacco/data_statistics/sgr/index.htm
58. Hurley S and Matthews J. The Quit Benefits Model: a Markov model for assessing the health benefits and health care cost savings of quitting smoking. Cost Effectiveness and Resource Allocation. 2007;5:2. Available from: http://www.resource-allocation.com/content/5/1/2
59. Brand DA, Saisana M, Rynn LA, Pennoni F and Lowenfels AB. Comparative analysis of alcohol control policies in 30 countries. PLoS Medicine. 2007;4:e151. Available from: http://medicine.plosjournals.org/perlserv/?request=getdocument&doi=10.1371/journal.pmed.0040151
60. Babor TF and Winstanley EL. The world of drinking: national alcohol control experiences in 18 countries. Addiction. 2008;103:721–5. Available from: http://www3.interscience.wiley.com/journal/119411977/abstract
61. Stockwell T. Australian alcohol policy and the public interest: a brief report card. Drug and Alcohol Review. 2004;23:377–9. Available from: http://www.informaworld.com/smpp/content~db=all?content=10.1080/09595230412331324491
62. Australia National Council on Drugs. April 2008 edition. Of Substance. 2008;6 Available from: http://www.ofsubstance.org.au/archive/pdf/ofsubstance_2008_4.pdf
63. Collins D and Lapsley H. The avoidable costs of alcohol abuse in Australia and the potential benefits of effective policies to reduce the social costs of alcohol. Canberra:
Department of Health and Ageing, 2008. Available from: http://www.nationaldrugstrategy.gov.au/internet/drugstrategy/publishing.nsf/Content/mono70
64. Australian Institute of Health and Welfare. 2007 National Drug Strategy Household Survey: first results. Drug Statistics Series, Number 20. Canberra: Australian Institute of Health and Welfare, 2008a. Available from:
http://www.aihw.gov.au/publications/phe/ndshs07-fr/ndshs07-fr-no-questionnaire.pdf
65. Dawe S, Frye S, Best D, Moss D, Atkinson J, Evans C, et al. Drug use in the family: impacts and implications for children. Research Paper 13. Australia National Council on Drugs, 2007. Available from: www.ancd.org.au/publications/pdf/rp13_drug_use_in_family.pdf
66. Government of Victoria Department of Human Services. An integrated strategy for child protection and placement services. Melbourne: Community Care Division, 2002. Available from: http://www.cyf.vic.gov.au/policy-planning-funding/library/publications/integrated_strategy
67. National Health and Medical Research Council. Australian alcohol guidelines for low-risk drinking. Canberra: National Health and Medical Research Council, 2007. Available from: http://www.nhmrc.gov.au/guidelines/_files/draft_australian_alcohol_guidelines.pdf
68. Chikritzhs T and Brady M. Fact or fiction? A critique of the National Aboriginal and Torres Strait Islander Social Survey 2002. Drug and Alcohol Review. 2006;25:277−87. Available from: http://www.informaworld.com/smpp/content~db=all?content=10.1080/09595230600644715
69. Ministerial Council on Drug Strategy. Towards safer drinking cultures: national alcohol strategy 2006-2009. Canberra: Ministerial Council on Drug Strategy, 2006.
70. Woolcott Research. Formative research for the development of a national alcohol social marketing initiative. Australian Government Department of Health and Ageing, 2007. Available from: http://www.alcohol.gov.au/internet/alcohol/publishing.nsf/Content/7C6B70D6091A3E4ACA25739A0082EFA5/$File/aaa-woolcottrep.pdf
71. Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht G, Grube J, et al. Alcohol: no ordinary commodity. New York: World Health Organization and Oxford University Press, 2003.
72. Henry K. Architecture of Australia’s tax and transfer system 2008. Available from: http://www.taxreview.treasury.gov.au/Content/downloads/report/Architecture_of_Australias_Tax_and_Transfer_System_Revised.pdf
73. Gluckman P, Hanson M, Cooper C and Thornburg K. Mechanisms of disease: effect of in utero and early-life conditions on adult health and disease. The New England Journal of Medicine. 2008;359:61–73. Available from: http://content.nejm.org/cgi/content/extract/359/1/61
74. Moodie R, Harper T and Oldenburg B. Options Paper for NHHRC: A national agency for illness prevention and health promotion. 2008. Available from: www.nhhrc.org.au
75. World Health Organization. Diet, nutrition and the prevention of chronic diseases: report of a joint WHO/FAO expert consultation. Geneva: World Health Organization, 2003. Available from: http://www.fao.org/docrep/005/AC911E/AC911E00.HTM
76. White V and Hayman J. Key results of the Victorian secondary school students’ use of licit and illicit substances in 2005 Results from the 2005 Australian Secondary Students’ Alcohol and Drug Survey. Victorian Department of Human Services. Centre for Behavioural Research in Cancer. Cancer Control Institute. The Cancer Council Victoria 2007.