Thinking Outside the Cell Defined Terms Baker's Dozen Problems Articles & Reports - Bibliography
Assisted dying for prison populations: Lessons from and for abroad - Dalhousie University, Canada - August 20, 2019
Authors - Jocelyn Downie, Adelina Iftene, Megan Steeves
Abstract
Canadian federal legislation setting out the framework for medical assistance in dying (MAiD) in Canada came into effect in June 2016. Because of section 86(1) of the Corrections and Conditional Release Act, as soon as MAiD became available in the community, it also needed to be made available to federal prisoners. There are some good reasons to be concerned about MAiD in the Canadian corrections system based on logistical, legal, and moral considerations. Fortunately, Canada is not the first country to decriminalize assisted dying and so Canadian policies and practices can be compared to others and take some lessons from their experiences. Thus, by reviewing the legal status of assisted dying in prisons internationally, the regulation of assisted dying, demand for assisted dying from prisoners, and the process for prisoners accessing assisted dying, this article offers a comparative overview of assisted dying for prisoners around the world in an effort to inform Canadian and other jurisdictions’ law, policy, and practice.
Introduction
In June 2016, medical assistance in dying (MAiD) became legal throughout Canada.1 Section 86(1) of the Corrections and Conditional Release Act (CCRA) requires the prison service to provide ‘essential health care’ to incarcerated individuals, therefore as soon as MAiD became available in the community, it also needed to be made available to federal prisoners.2 By September 2017, there had been eight requests for MAiD from people incarcerated in the federal system.3 The number of requests will likely increase given the aging of the prison population (as more people enter prison at an older age, leave prison at older ages, or stay until they are older and die in prison) and the phenomenon of “accelerated aging” in prisons (as incarcerated individuals tend to present the health problems of people in the community who are 10–15 years older).4 In November 2017, Correctional Service Canada (CSC) released a guideline establishing its operational directive for MAiD.5 According to the Office of the Correctional Investigator (OCI) Annual Report 2017–2018, the first case of MAiD for a Canadian prisoner has now occurred.6
There are good reasons to be concerned about MAiD in the Canadian corrections system. These include, for example:
-
the possibility that the first case of MAiD for a Canadian prisoner involved one physician providing both of the two required assessments of eligibility (contrary to the federal legislation) and that the MAiD provider was not sufficiently independent of CSC (contrary to the CSC Guideline)7;
-
the possibility that the inadequacies of the mechanisms for release or transfer into community for assessments, provision, and decision-making regarding MAiD may result in lack of access for those who are eligible under the legislation; and
-
the moral complexities of implementing MAiD in a context within which voluntariness, information, and access to end of life care have not been adequately analyzed; and where access to general health care has been documented to be inadequate.8
Fortunately, Canada is not the first country to decriminalize assisted dying and so we can compare our policies and practices to others and take some lessons from their experiences. We can also, in turn, offer lessons based on our experiences to the increasing number of jurisdictions considering the decriminalization of assisted dying.9
In Part 1, we discuss the legal status of assisted dying in prisons internationally, the regulation of assisted dying, demand for assisted dying from prisoners, and the process for prisoners accessing assisted dying. In Part 2, we draw lessons from jurisdictions that permit assisted dying by reflecting on how they have grappled with the implementation of assisted dying for prisoners. In sum, in this article, we offer a comparative overview of assisted dying for prisoners around the world in an effort to inform Canadian and other jurisdictions’ law, policy, and practice.
Before doing so, however, we must explain the terminology used in this article and provide a brief overview of the most recent and transformative steps on the journey to legalizing MAiD in Canada.
Different jurisdictions use distinct terms to refer to various forms of assisted dying. In Canada, we use “medical assistance in dying” (MAiD) as an umbrella term to capture both provider-administered and self-administered assistance in dying.
MAiD means:
-
the administering by a medical practitioner or nurse practitioner of a substance to a person, at their request, that causes their death; or
-
the prescribing or providing by a medical practitioner or nurse practitioner of a substance to a person, at their request, so that they may self-administer the substance and in doing so cause their own death.10
Other jurisdictions use a range of other terms including -
-
suicidio asistido and eutanasia (Colombia),
-
levensbeeindiging op verzoek (ending of life on request) and hulp bij zelfdoding (assisted suicide) (the Netherlands),
-
voluntary assisted dying (Victoria, Australia); and
-
aid in dying (many US states).
Conceptually, these all map onto either self-administered or provider-administered assisted dying. In this article, we use MAiD to refer to assisted dying specifically in Canada, “assisted dying” to refer to both self- and provider-administered assistance in dying in other jurisdictions that allow both kinds of assisted dying (including Canada when not referring solely to Canada), and “provider-administered assistance in dying” and “self-administered assistance in dying” when referring to only one of the two kinds of assisted dying.
In February 2015, the Supreme Court of Canada in Carter v. Canada (Attorney General) 11 ruled that the Criminal Code of Canada prohibitions on MAiD violated the Canadian Charter of Rights and Freedoms. 12 In response to this decision, the federal government passed amendments to the Criminal Code to establish the legal framework for MAiD in Canada.13 A competent adult can access MAiD if they have made a voluntary request and have a “grievous and irremediable medical condition”14 (which does not require a terminal illness or a finding of temporal proximity to death). Physicians and nurse practitioners can provide MAiD, and MAiD can be provider- or self-administered. It should also be flagged that Quebec is unique in Canada insofar as there is provincial legislation governing MAiD which came into force before the federal legislation and is narrower in scope (e.g. it allows only physician provision and only provider- and not self-administered MAiD and it requires that the person be at the “end of life” in order to be eligible).15
Part I: Assisted dying in the prison context around the world
Assisted dying legislation and guidelines
Currently, 15 jurisdictions allow the practice of assisted dying. Six of these jurisdictions are countries (Belgium, Canada, Colombia, Luxembourg, the Netherlands, and Switzerland). Eight are jurisdictions within the United States (California, Colorado, the District of Columbia, Hawaii, Montana, Oregon, Vermont, and Washington) and one is a state in Australia (Victoria).16 The prison context is not mentioned in any assisted dying law in any jurisdiction with the exception of Canada.17 No law explicitly excludes prisoners from accessing assisted dying or describes a different legal framework for assisted dying that is specific to prisoners. We found no official guidelines specifically regulating assisted dying in prisons in any permissive jurisdiction, with the exception of Canada.18
The legal requirement to make assisted dying available to prisoners in a permissive regime
Once assisted dying has been decriminalized, in many jurisdictions, it must be made available to a country’s prison population because of the principle of equivalence of care. This principle establishes that a country’s prisoner population must be provided with health care that is equivalent to what members of that country’s general population receive.19 This principle has received international recognition and is included in the Standard Minimum Rules for the Protection of Prisoners (known as the Mandela Rules), one of the main United Nations guidelines for the protection of prisoners.20
In Canada, section 86 of the CCRA requires that essential health care (including mental health care) be provided to the prison population, and that the prison population have reasonable access to nonessential health services.21 The Act also stipulates that the provision of these services must conform with professionally accepted standards.22 In addition, there is a common-law duty of care, which includes the duty to provide health care.23
It is important to note here that MAiD in Canada is treated as a form of health care—it is delivered by medical and nurse practitioners24 and is funded by the provincial/territorial health systems in the same way other health services are funded.25
Internationally, besides the Mandela Rules, there are various regional and national guidelines describing the principle of equivalence, and its role as the benchmark for the minimum standard of care that should be met in prison medicine. The Council of Europe, of which Belgium, Luxembourg, and the Netherlands are members, has set standards for prison medicine.26 These standards make explicit reference to equivalence of care. The principle shares a similar position in the American prison system, although it has only been recognized in case law exploring prisoners’ rights to medical care.27 Again, it is important to note that, as in Canada, assisted dying is treated as a form of health care in these jurisdictions. That is, in these jurisdictions, assisted dying is provided by physicians within the physician–patient relationship and is covered by the health insurance system.
It therefore appears that Canada, Belgium, Luxembourg, the Netherlands, and the United States must ensure that prisoners can access assisted dying.
The demand for assisted dying from prisoners
Given that assisted dying is now legal and must be made available to individuals in prisons in some jurisdictions, the next question to ask is whether there is any demand for it within the prison context.
Demand in Canada
Complete and reliable information about MAiD in Canadian prisons is not readily available. Information that CSC disclosed on July 7, 2018, in response to a freedom of information request indicated that, as of September 17, 2017, only one prisoner had met the eligibility criteria for MAiD, but they passed away before the procedure could be provided.28 CSC did not disclose the number of requests made (despite this information having been requested). In March 2018, CBC News reported that eight Canadian prisoners had requested MAiD, three had been deemed eligible for MAiD, and two of these eligible persons had not yet received the procedure, but were living in the community.29 No information is available on the reasons for prisoners having been deemed ineligible or about the underlying medical conditions of the one deemed eligible. The 2017–2018 Annual Report of the OCI reported that one prisoner had received MAiD.30
While complete and reliable data regarding actual demand for MAiD in prisons is not yet available, given the demographics of the Canadian prison population, it is reasonable to assume that there will be demand. The number of Canadian prisoners aged 50 years and older is growing,31 and, in 2016, this group made up about one-quarter of the federal prison population.32 The latest data available indicates that the average age at death was 60.33 which is significantly lower than the average life expectancy outside prison at 82.34 The leading causes of prisoners’ deaths were cancer, cardiovascular illness, respiratory diseases, liver issues, and infections.35
In Canada, 3714 MAiD deaths were reported among members of the general population between December 2015 and December 2017.36 On average, recipients of MAiD were 73 years old, and roughly one half were male.37 The most common underlying medical conditions between July 2017 and December 2017 were cancer-related (65%), circulatory/respiratory (16%), neuro-degenerative (10%), and other (9%).38
Given the age and burden of disease for prisoners dying behind bars and the underlying medical conditions of individuals receiving MAiD outside the prison context, it is reasonable to conclude that MAiD requests will come from the prison population and that a number of those who request MAiD will meet the eligibility criteria.
Demand in other permissive jurisdictions
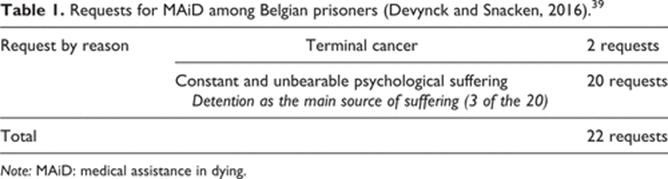
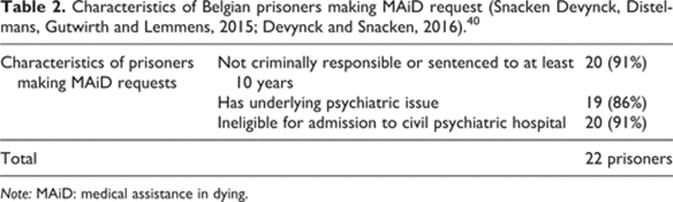
Internationally, there is some information available about assisted dying requests among prisoners, primarily among Belgian (See Table 1, 2 and 3) and Swiss prisoners.
{kind=link}
|
{kind=link}
{kind=link}
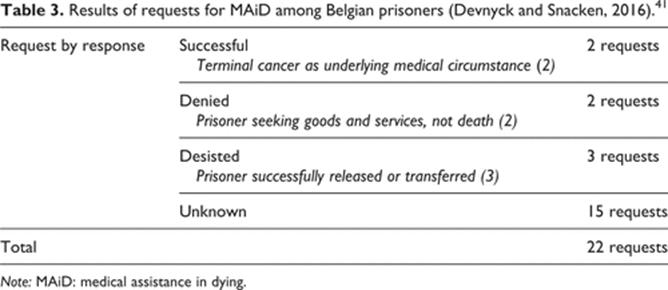
Based on the information available about assisted dying requests in Belgium, it appears that assisted dying is being viewed by prisoners (20 (91%)) as a means to end psychological suffering.42 Notably, some prisoners who sought assisted dying (3 (15%)) attributed their psychological suffering to incarceration itself,43 and this is not surprising given its well-documented negative impact on one’s psyche.44 However, only requests involving a physical health condition as the underlying medical circumstance (2) have been granted for Belgian prisoners.
Researchers in Switzerland have found that Swiss prisoners also report interest in exploring self-administered assisted dying as a means to end psychological suffering.45 An unspecified number report having attempted to contact ‘Exit’, a self-administered assisted dying provider, but not having received a reply.46 Interestingly, Exit’s president reports never receiving any requests from a prisoner, although he sees no objection to fielding such requests.47 It seems reasonable to conclude that there is an unmet demand for self-administered assisted dying among Swiss prisoners.
In the other permissive jurisdictions, the available information either states or implies that no requests for assisted dying have been made among the prison population.48 There are no reports of assisted dying having been accessed by prisoners in these other permissive jurisdictions.
It should be noted that some scholars have suggested that the lack of requests from prisoners in jurisdictions where assisted dying is available for non-prisoners could be due to the fact that this service, while legally permissible, is not actually available to prisoners,49 and hence the requests are not monitored. If that is the case, the apparent lack of requests should not be taken as indicative of demand.
The process for prisoners accessing assisted dying
Having established that where assisted dying is now legal, it must also be made available to prisoners in some jurisdictions, and that some prisoners will want to access it, we turn now to exploring the process for prisoners accessing assisted dying.
Process in Canada
According to the CSC Guideline, a federal prisoner seeking MAiD must submit a request to the institution’s Health Services. Within 5 days of submitting the request, they will be seen by the Chief of Health Services or the institutional physician or nurse practitioner, who will provide them with information regarding MAiD and, if requested, schedule a first eligibility assessment. This will be conducted by the prison physician or nurse practitioner. The prisoner does not have a choice of assessor and, unlike individuals outside the corrections context, cannot seek a second opinion if the first assessor believes the eligibility criteria are not met.
If the first assessor believes the criteria are met, “all release options will be considered”50 (under the CSC Guideline, mechanisms for “release” include parole by exception, the royal prerogative of mercy, and temporary absence51). If the prisoner is granted parole or given a pardon, then they will be released into the community and their health care will no longer be under the authority or be the responsibility of CSC. They will need to seek access to MAiD or alternatives to MAiD in the same way as anyone else in the community. If they have been denied parole or a pardon or if they are awaiting a decision on parole or pardon and cannot delay the MAiD process until that decision comes, they will need to continue to seek access to MAiD or alternatives to MAiD through CSC.
If the first assessor believes the prisoner meets the eligibility criteria, then the prisoner will undergo a second assessment conducted by an external physician or nurse practitioner usually in the community through the “temporary absence” mechanism.52 If both assessors are of the opinion that the eligibility criteria are met, then the prisoner will be provided with the procedure, usually in the community, again through the “temporary absence” mechanism after the required 10-day waiting period (or less if death or the loss of capacity are imminent). The Guideline assumes that most of the time the second assessment will take place in the community53 and assumes that most of the time MAiD will be provided external to CSC, namely, in a community hospital or other location. In exceptional circumstances, at the request of the prisoner, MAiD may be provided in a prison or CSC regional hospital if:
· an exception has been approved by the Assistant Commissioner, Health Services; and
· the procedure includes a health professional external to CSC.54
Process in other permissive jurisdictions
Despite the lack of a formal guideline in other permissive jurisdictions, some Belgian and Swiss scholars have written about the procedures surrounding MAiD in prisons in practice (Table 4).
|
{kind=link}
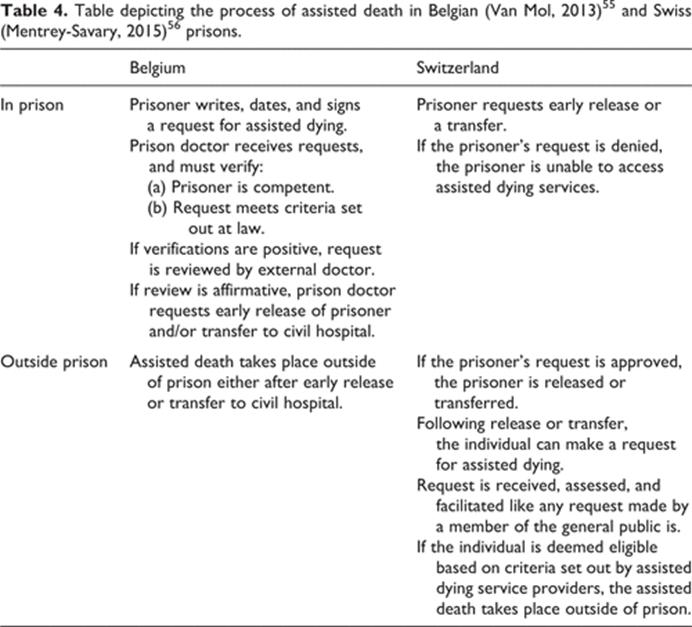
The Belgian approach uses prison doctors to assess MAiD eligibility. These doctors are positioned to facilitate the assisted dying process. Assisted dying appears to have been integrated into the Belgian prison health system (albeit with provision occurring outside the prisons). In contrast, the Swiss approach requires that prisoners first leave the prison environment before they are able to be assessed for or to access self-administered assisted dying.57 There are no assessments for, or facilitation of, self-administered assisted dying by prison officials in Swiss prisons. Self-administered assisted dying can, theoretically, only be assessed/accessed once a prisoner has been released or transferred.58
Given the connection between the process for accessing assisted dying and general release or transfer mechanisms, it is necessary here to explain these processes and mechanisms in greater detail in order to illuminate some significant barriers to accessing assisted dying facing prisoners in many seemingly permissive jurisdictions59 and some implications for the voluntariness of the decision to access MAiD.
If assisted dying is available in prisons and in the community, then the mechanisms for release or transfer into community will affect a prisoner’s ability to access assisted dying in their preferred location. If assisted dying is only available in community, then access will be contingent on prisoners’ ability to be released or transferred into community. Therefore, in order to assess the availability of assisted dying for prisoners, it is essential to contrast the eligibility criteria for assisted dying with the eligibility criteria for release or transfer into community.
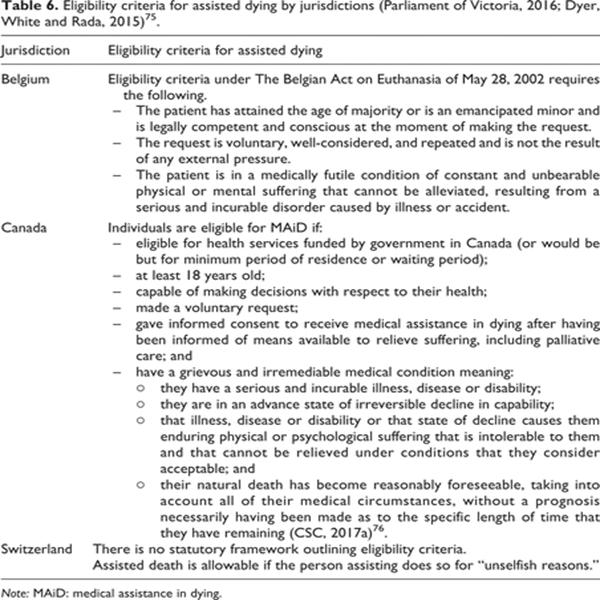
A comparison of Tables 5 and 6 reveals that the eligibility criteria for assisted dying and the eligibility criteria for release or transfer into community are not the same, and thus, it is possible for a prisoner to be eligible for assisted dying and ineligible for release or transfer into community. For example, a prisoner could be eligible for assisted dying in Canada because of a grievous and irremediable medical condition but be ineligible for release into community because they pose a safety risk to others.

|
{kind=link}
In addition, in Canada, release through parole by exception or pardon is rare to nonexistent, respectively, and the application process is cumbersome, time-consuming, and restrictive. The procedure for applying for release through a temporary absence is more accessible, and temporary absences are more common than parole by exception or pardons. However, the temporary absence mechanism is vulnerable to the lack of availability of services or beds in the community and to the costs of escorts for escorted temporary absences. Thus, it is more likely to be for short durations if at all. For example, there might be sufficient availability for a bed and escort for a day for MAiD but not a bed and escort for 6 months for palliative care. Also, unlike when a person is released on parole or pardoned, when a person is released on a temporary absence for MAiD, if they change their mind, they will be returned to prison.
In sum, if assisted dying is not available within the prison setting, the practical hurdles of the release or transfer application processes and the restrictive eligibility criteria for release or transfer into community may be barriers to access to assisted dying. If assisted dying is available in prison, the coercive and oppressive environment of prisons may be a barrier to truly voluntary decision-making about assisted dying. If assisted dying is only available outside prisons through a temporary absence mechanism, assisted dying may be more accessible than palliative care and therefore the voluntariness of the choice between assisted dying and palliative care may be compromised.
Part 2: Lessons learned
A number of issues have surfaced from this review of the experience to date with assisted dying in prisons in jurisdictions that permit some form of assisted dying. These are relevant for permissive jurisdictions as they seek to implement or manage assisted dying for prisoners. They are also relevant for other jurisdictions that are exploring the decriminalization of assisted dying or as they design and implement a permissive assisted dying regime.
Equivalence of care
Countries that have embraced the principle of equivalence of care must wrestle with the implications of this principle for decriminalizing assisted dying. That is, if a jurisdiction has embraced the principle and decriminalizes assisted dying, they will be obliged to ensure access to assisted dying for prisoners (whether in the community or in the prison). Alternatively, they will need to include and justify an explicit exception regarding access within their legislation.
Countries appear to have failed to meet the principle of equivalence of care in the context of assisted dying. The fact that there are so few documented requests for, and provision of, MAiD given the age and burden of disease among prisoners compared to the number of requests and provision of MAiD in the general population suggests that the principle is not being met. CSC’s position that a prisoner cannot seek a second assessment if the first assessor determines they are not eligible is a clear breach of this principle.
The interaction of eligibility criteria for assisted dying and for release or transfer into community
Policy-makers must be alive to the interaction of eligibility criteria for assisted dying and for release into community. This is not to suggest a particular position on the prioritization of the criteria. Rather, it is to flag that restrictive release criteria (especially non-health–related criteria) will mean that there will be more prisoners who are eligible for assisted dying seeking assisted dying within the walls of the prison (and this then links back to the issue of equivalence of care). If assisted dying is not available within the walls of the prison and if the eligibility criteria for release to community leave prisoners who are eligible for assisted dying in prison, policy-makers will be responsible for this violation of the principle of equivalence. Restrictive release criteria (again especially non-health–related ones) also make it all the more essential to wrestle with the ethical concerns about voluntariness raised by many about the provision of assisted dying inside prisons or through temporary absence/transfer rather than release (through, e.g. parole or the Royal Prerogative of Mercy).
Psychological suffering
Unbearable psychological suffering formed the basis of most prisoners’ assisted dying requests internationally.77 Some have suggested that this is an indication that prisons have failed to provide adequate mental health services to their populations78 and have suggested that steps can and should be taken to reverse this trend.79 At the very least, this suggests that permissive assisted dying regimes should wrestle with the role of psychological suffering as a basis for assisted dying. Specifically, what is the relevance of the fact that at least some of a prisoner’s psychological suffering is likely due to the conditions of imprisonment and/or the lack of access to mental health services in prisons?
Education
As noted earlier, older Canadian prisoners report being unaware of the release options available to them.80 Health literacy among prisoners is low81 and can be compounded by a lack of communication between assisted dying service providers and the prison population.82 In permissive jurisdictions, prisoners, and especially those who are aging behind bars, must be educated about assisted dying and other end of life care options as well as the release mechanisms that may be available to them. The design of education programs must, of course, be sensitive to the risk of inducing requests for MAiD.
Conclusion
Recent developments in assisted dying have raised new challenges for health and legal professionals, as well as prison administrators and staff. Attention must clearly be paid to the ramifications of the decriminalization of assisted dying practices on marginalized populations. This is especially true for prisoners given the increasing number of older individuals in prisons. This article aimed to provide a synopsis of the current state of assisted dying in prisons in permissive jurisdictions around the world in order to highlight issues that must be attended to by those who have decriminalized or are considering decriminalizing assisted dying. Lessons learned by those who have already had some experience with assisted dying in prisons are offered.